Download
1 / 26
290 likes | 470 Views
Vitamin D. Zulf Mughal Consultant in Paediatric Bone Disorders Department of Paediatric Endocriology Royal Manchester Children's Hospital Manchester M13 0JH. Bone Study Day, 28 th September 2012. Overview. Sources & Metabolism of Vitamin D

E N D
Vitamin D Zulf Mughal Consultant in Paediatric Bone Disorders Department of Paediatric Endocriology Royal Manchester Children's Hospital Manchester M13 0JH Bone Study Day, 28th September 2012
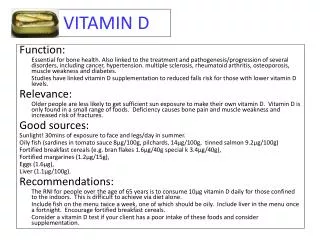
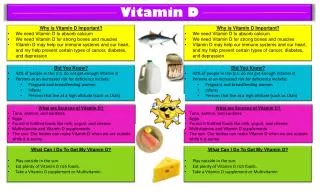
Overview • Sources & Metabolism of Vitamin D • Musculoskeletal consequences of Vitamin D deficiency • Non-musculoskeletal associations of Vitamin D deficiency • The Criteria or Definition of Vitamin D deficiency • Prevention of Vitamin D deficiency
Solar UVB (280-310nm) Endogenous Vitamin D3 Liver 25-Hydroxyvitamin D (major circulating metabolite) Dietary source Vitamin D2 & D3 • Oily fish, eggs, • fortified foods e.g: • Infant formulas • Cereals 1,25-Dihydroxyvitamin D Sources & Metabolism of Vitamin D DBP 25-hydroxylase (CYP2R1) (7-dehydoxycholesterol) DBP Kidney 24,25-hydroxyvitamin D • PTH (+) • ↓ P (+) • FGF23 (-) 1α hydroxylase (CYP27B1) 24-hydroxylase (CYP24A1) Calcitroic acid
Roles of 1,25-Dihydroxyvitamin D in Bone Mineral Homeostasis • Stimulates GI calcium absorption • Promotes renal calcium re-absorption • Stimulates GI phosphorous absorption • Calcium homeostasis: together with PTH it mobilises calcium from skeletal stores • Mineralisation of the growth plate & osteoid Low Calcium or Low Phosphorous Radiograph showing Rachitic Changes Normal Growth Plate Rachitic Growth Plate
Factors which contribute to development of Vitamin D deficiency • Residence in Northern or Southern Latitudes • Pigmented skin • Sun blocking creams – Factor 8 ↓ Vit D synthesis by >95% • Sunshine avoidance for religious or cultural reasons • Cloud Cover & Atmospheric Pollution • Obesity • Genetic propensity • An independent protective effect of meat consumption • Low dietary Calcium & High Fibre diets
Maternal & Cord 25-Hydroxyvitamin DConcentrations R=0.98 (p<0.001) N = 22 Lau 2001 (Unpublished) Vitamin D stores acquired during fetal life last ~ 8 weeks
Serum 25(OH) Levels after Simulated Summer Sunlight Exposures in Whites & South Asians South Asians need 4 times longer Exposure 2 Hours of Summer Sunlight Exposure 3 x Week 109 Whites 15 South Asians Farrar et al Am J Clin Nutr. 2011;94(5):1219-24.
Vitamin D Deficiency & Insufficiency Definition of vitamin D deficiency & sufficiency based on serum 25(OH)D concentrations Davies JH & Shaw NJ. Arch Dis Child. 2010 Jul 23. [Epub ahead of print]
Low Calcium Diet & Vitamin D Deficiency Khadilkar, Das, Sayyad, Sanwalka, Bhandari, Khadilkar, Mughal. Low Calcium intake & Hypovitaminosis D in Adolescent Girls. Archives of Disease in Childhood. 2007 ;92(11):1045
Low Calcium & High Fibre Diet and Vitamin D Status • High fibre & phytic acid reduce dietary Ca intake • Low Ca intake leads to secondary hyperparathyroidism & raised serum 1,25(OH)2D concentration • Raised serum 1,25(OH)2D concentration degrades 25OHD to inactive 24,25-dihydroxyvitamin D, thereby depleting body stores of vitamin D Clements et al. Nature 1987;325:62–5 Vitamin D Dietary Ca
DIETARY CALCIUM INTAKE 1 ml ~ 1mg RNI (mg/day) in the UK Infants up to 1 yr 525 Children 1- 3 yrs 350 Children 2-6 yrs 450 Children 7-10 yrs 550 Adolescent boys 11-18 yrs 1000 Adolescent girls 11-18 yrs 800 1 oz ~ 200 mg 1 pot ~ 150 mg ~35 mg/slice 1 Bowl ~ 80 mg
Vitamin D Deficiency & Myopathy 8th April 09 5th May 09 • 14 year old female • Limb pains • Difficulty walking & Climbing stairs • Life long intolerance of dairy products (Ca intake <300 mg/day) • Arrived from Saudi Arabia 8 months ago DIAGNOSIS: Severe vitamin D deficiency & low calcium intake Rx:Single orally dose 180, 000 IU Vitamin D3 + 500mg/day Ca supplement
Life threatening Cardiomyopathy in Early Infancy • 16 infants (6 South Asian, 10 Black ethnicity) admitted to GOS with Heart Failure • Median age 5.3 months (3 weeks - 8 months);12 exclusively breast-fed • 12 needed inotropic support • 8 ventilated & 2 needed ECMO • 2 referred for cardiac transplantation • 6 suffered a cardiac arrest & 3 died! Median (range) Reference range Calcium (mmol/L) 1.50 (1.07 – 1.74) 2.17 – 2.44 PTH (pmol/L) 34.3 (8.9 – 102) 0.7 – 5.6 25OHD (nmol/L) 18.5 (0.00 – 46) >50 Fractional shortening (%) 10 (5-18) 28 – 45 Left ventricular end diastolic dimension Z score 4.1 (3.1-7) -2 < +2 Maiya S et al .Hypocalcaemia and Vitamin D deficiency: an important, but preventable cause of life threatening infant heart failure.Heart. 2007 Aug 9; [Epub]
Possible Consequences of Vitamin D Deficiency Holick BMJ June 2008;336:1318-1319
Vitamin D & Innate Immunity • Innate immunity • Toll like receptors recognise pathogens • expression of VDR & CYP27B1 enzyme 25(OH)D 1,25(OH)2D • 1,25(HO)2D leads to production of antimicrobial proteins (AMPs) • AMPs (e.g. Cathelcidin) important role in defence against bacterial & viral infections Adequate serum 25(OH)D
Vitamin D Deficiency & Pneumonia New RMCH July 2009
Effects of Vitamin D supplementation in children diagnosed with pneumonia in Kabul: A randomised controlled trial Proportion of children free of a repeat episode of pneumonia up to 90 days post-treatment Rx of 1-36 month olds with 100,000 i.u. Vitamin D3/Placebo + antibiotics • DID NOT reduce the duration of illness (p=0.17) • DID reduce readmission to hospital with pneumonia (p=0.01) Manaseki-Holland S, Qader G, Masher M I, Bruce J. Mughal M Z, Chandramohan D, Walraven G, Effects of Vitamin D supplementation to children diagnosed with pneumonia in Kabul: A randomised controlled trial. Tropical Medicine & International Health 2010;15 (10), 1148–1155
Vitamin D Supplementation to Infants in Kabul had NO effect on the incidence of Pneumonia: A randomised controlled trial Proportion of Children without First or Only Episode of X-Ray Confirmed Severe & Non-Severe Pneumonia • 3,406 infants randomised to 100,000 i.u. Vitamin D3 or Placebo every 3-monthly, for 18 months • Subjects visited fortnightly to assess their health status • Subjects with signs of pneumonia had a chest radiograph to confirm the diagnosis of pneumonia. • No difference in the incidence of pneumonia between the vitamin D and the placebo group Manaseki-Holland, Maroof, Bruce, Mughal, Masher, Bhutta, Walraven, Chandramohan Effect on the incidence of pneumonia of vitamin D supplementation by quarterly bolus dose to infants in Kabul: a randomised controlled superiority trial LANCET .2012;14;379(9824):1419-27
Summary • Subclinical vitamin D deficiency is very common in the UK • Severe vitamin D deficiency is associated skeletal muscle weakness & cardiomyopathy. • No clear definition of vitamin D deficiency based on serum 25(OH)D levels in children. • Pragmatic lower limit of vitamin D sufficiency – 20 ng/ml or 50 nmol/l. • Adequate dietary calcium intake is important in order to prevent vitamin D breakdown. • Musculoskeletal symptoms of vitamin D deficiency are less likely to occur when dietary calcium intake is adequate & serum PTH is normal. • Vitamin D deficiency may be associated with increased risk of infections, autoimmune disorders, respiratory diseases & certain cancers. RCTs needed to confirm these associations!
Thank You zulf.mughal@cmft.nhs.uk