Download
1 / 26
410 likes | 1.55k Views
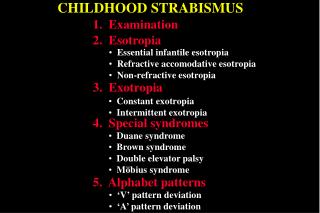
Duane’s Syndrome. Violent Violation of Sherrington’s Law. Definition. Disturbance of ocular movement characterized by simultaneous contraction of the medial and lateral rectus muscles in adduction. History. 1879 - Heuck describes a case of retraction in adduction 1887 - Stilling

E N D
Duane’s Syndrome Violent Violation of Sherrington’s Law
Definition Disturbance of ocular movement characterized by simultaneous contraction of the medial and lateral rectus muscles in adduction
History 1879 - Heuck describes a case of retraction in adduction 1887 - Stilling 1895 - Sinclair 1896 - Bahr 1899 - Turk 1900 – Wolff 1905 - Duane presents 54 collected cases Duane's known as Stilling-Turk-Duane Syndrome in Europe
Prevalence • Types I, II, and III • Incidence 1-4 percent of all strabismus • Female 54-62% • Left eye 60-75% where unilateral • Bilateral 18-22% • Many associated congenital anomalies • Occasionally familial
Diagnostic Features • Reduced abduction • Retraction of the globe on adduction • Co-contraction of the lateral and medial recti on adduction
Associated Features • Upshoot or downshoot in adduction • Narrowing of palpebral fissure - minimal in some cases • Low angle esotropia or exotropia • Head turn for fusion • "Y" or "V" pattern • Synergistic divergence
Differential Diagnosis • Abducens palsy - usually larger angle esotropia in primary gaze • Ocular myasthenia • Spasm of the near reflex • Medial rectus entrapment with medial orbit wall fracture • Strabismus fixus • Ocular neuromyotonia • Graves ophthalmopathy
Duane’s-Associated Syndromes33% of All Duane’s • Klippel-Feil Anomaly 3-4% • Labyrinthine deafness 8-16 % • Wildervanck Syndrome both of above • Goldenhar Syndrome • Crocodile tears • Arthrogryposis multiplex congenita • Marcus-Gunn Jaw Winking Syndrome • Many others
Etiology Neuroanatomy • 1. Deficient innervation of lateral rectus • 2. Innervation of lateral rectus by anomalous branch of 3rd nerve • 3. Brainstem origin Embryology • 1. Teratogenesis at 8 weeks gestation • 2. Absence of abducens motor neurons
Type I Duane’s • Most Common – 78% • Very reduced abduction • Globe retraction with attempted adduction • Narrowing of palpebral fissure with adduction • Typically esotropic • Absent sixth nerve nucleus
Type II Duane’s • Least common -7% • Fair abduction • Reduced adduction • Globe retraction and narrowing of palpebral fissure with adduction • Often Exotropic
Type III Duane’s Syndrome • Incidence about 15% • Poor abduction and adduction • Globe retraction and narrowing fissure in adduction • Minimal deviation in primary gaze • Tonic firing of horizontal rectus muscles
Secondary Effects of Duane’s • Pseudo-overaction of inferior oblique • Due to leash effect of contracting LR • V, Y and X patterns • Face turn
Treatment of Duane’s • Rationale for treatment • Disruptive head turn • Diplopia (rare) • Suppression and amblyopia (uncommon) • Large angle deviation in primary gaze • Deviation in up or downgaze • Treatment modalities • Many cases require no intervention • Prism in spectacles • Surgery
Surgery-Type I • For minimal co-contraction do large ipsilateral MR recession • For severe co-contraction-small ipsilateral MR recession and large contralateral MR recession • Avoid lateral rectus resection • Approach transposition with caution because of vertical deviations
Recession MEDIAL RECTUS
Surgery for Type II • Ipsilateral lateral rectus recession • Contralateral medial rectus resection
Surgery for Type III • Fadenoperation on Contralateral medial rectus and lateral rectus
Surgery for Upshoot or Y-pattern • Y-splitting of lateral rectus • Fadenoperation of lateral rectus
Bilateral Duane’sDanger of consecutive XT • Simultaneous recession of medial and lateral rectus M.R