Download
1 / 44
440 likes | 624 Views
Depression in Adolescents. Charles D. Casat, M.D. Director of Research Behavioral Health Center Carolinas HealthCare System Charlotte, NC. Spectrum of Depressive Disorders in Adolescents. Major Depressive Disorder (MDD) Minor Depressive Disorder Dysthymic Disorder Bipolar Disorder (BPD)

E N D
Depression in Adolescents Charles D. Casat, M.D. Director of Research Behavioral Health Center Carolinas HealthCare System Charlotte, NC TADS
Spectrum of Depressive Disorders in Adolescents • Major Depressive Disorder (MDD) • Minor Depressive Disorder • Dysthymic Disorder • Bipolar Disorder (BPD) • Adjustment Disorder with Depressed Mood TADS
Prevalence of Depressive Disorders (Birmaher et al, 1996) • Community studies of depression in non-referred adolescents indicate: • MDD-- 0.4% to 8.3% • Dysthymia-- 1.6% to 8.0% TADS
Sex Ratios in Adolescent Depression • The ratio of depressed females to males is approximately 2:1 beginning at about 12 years of age • Explanation for sex differences includes: • socio-cultural factors • biological changes with puberty • predisposition to anxiety disorders • cognitive predisposition TADS
Secular Trend in Depressive Disorders • In the latter 20th century, those later-born generations have a greater risk • Depression is occurring at an earlier age than previously • The increase may be due to environmental factors, or an interaction between environment and genetic factors TADS
Age at Onset and Lifetime Family Risk for Depression Group: 1° Relatives Risk: Prepubertal onset (Puig-Antich et al, 1988) .50 Adolescent-onset (Strober et al, 1988) .35 Adult-onset (Gershon et al, 1982) .18-.30 TADS
Family Aggregation of Disorders in Adolescent MDD • Relatives of adolescents with MDD showed increases in: (Klein, Lewinsohn, Rohde et al, 2001) • Major Depressive Disorder (HR= 1.77) • Dysthymia (HR= 1.79) • Alcohol Abuse (HR= 1.29) • No increase in anxiety disorders, drug abuse, antisocial disorder, or borderline personality TADS
Adolescent Depression and Bipolar Disorder Outcome Strober and Carlson (1988) 20% Kovacs et al (1988) 20% Geller et al (1994) 32% Rao et al (1994) 19% TADS
MDD and Occurrence of Comorbid Diagnoses Investigator: (n=) Conduct/ Anxiety ODD Disorder Puig-Antich (28) 37% 48%-59% Kovacs (29) 17% 33% Mitchell (45) 16% 11%42% Alessi (28) 40% 48% TADS
The Effects of Comorbidity May Include: • The time at which a disorder is diagnosed • Outcome anticipated with/without treatment • The choice of treatment(s) • The level of functional impairment expected TADS
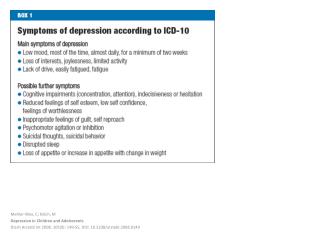
Criterion Symptoms in MDD (1) A. Five or more symptoms that have been present in the same 2-week period, and represent a distinct change of functioning One symptom must be either: 1. Depressed mood, most of the day, nearly every day 2. Markedly diminished interest or pleasure in all, or almost all activities TADS
Criterion Symptoms in MDD (2) 3. Significant weight loss 4. Insomnia or hypersomnia 5. Psychomotor agitation or retardation 6. Loss of energy or fatigue 7. Feelings of worthlessness or guilt 8. Diminished ability to think or concentrate 9. Recurrent thoughts of death or suicide TADS
Criterion Symptoms in MDD (3) B. The symptoms do not meet criteria for a Mixed Episode of Bipolar Disorder C. The symptoms cause clinically significant distress or impairment D. The symptoms are not due to the direct physiological effects of a substance, or other general medical condition E. Not better accounted-for by bereavement TADS
Assessment and Diagnosis in Adolescent Depression • Assessment is multi-trait, multi-informant • clinical interview • symptom rating scales • personality inventories • structured diagnostic interviews • Diagnosis can be made using the unmodified DSM-IV criteria TADS
Assessment Instruments • Symptom rating scales: CDI, BDI, CDRS, CES-D • rating scales do not establish diagnosis, but correlate with diagnosis by other means • Behavioral Inventories: YSR, BASC, PIC • Structured Diagnostic Interviews: DICA, DISC, K-SADS-PL • Systematic inventories of DSM criterion SX TADS
An Overview of Management of Adolescent Depression (1) • Psychoeducation for the patient and family • Linking the family with support groups (NAMI, MHA, DMDA) • Development of age-appropriate social skills • Development of problem-solving skills and self-evaluation and self-monitoring skills TADS
An Overview of Management of Adolescent Depression (2) • Mood-elevating and other medications • Stress identification and management • Vigorous management of comorbid S/A, internalizing and externalizing disorders • Assessment and management of suicidal behaviors TADS
Pharmacologic Treatment of Adolescent Depression Imipramine Fluoxetine Phenelzine Amitriptyline Sertraline Desipramine Paroxetine Bupropion Nortriptyline Citalopram Mirtazapine Clomipramine Fluvoxamine Venlafaxine Nefazadone Trazodone TADS
Efficacy of Tricyclics in Children and Adolescents • A meta-analysis of 12 placebo-controlled trials of TCA’s in patients 8-16 years of age found no advantage over placebo (Hazell et al, 1995) TADS
Explanations for Lack of TCA Efficacy (Emslie et al, 1997) • definition of response • small sample sizes • length of treatment • comorbidity • heterogeneity • varying symptom severity • noradrenergic system immaturity • large placebo response (33%-68%) TADS
Efficacy of Fluoxetine in C/A MDD (1) (Emslie et al, 1997) • 96 outpatients, stratified 8-12 yrs and 13-17 yrs • Randomized, double-blind, PBO-controlled • Primary outcome measures: CDRS and CGI • The age group-by-treatment was ns. (p= .76) • Response rate: FLU= 56%, PBO= 33% • CDRS ANOVA (n= 96) was p= .01 • CGI-I of “1” or “2” improved (K-M = .017) • More drop-outs in PBO group TADS
Emslie et al, 1997 (Emslie et al, 1997) TADS
Efficacy of Paroxetine in MDD in Adolescents • Multi-site, randomized, placebo-controlled trial of 275 adolescents, 12-19 years, with MDD % Responders • Paroxetine up to 40 mg/day 66%% p<.05 • Imipramine up to 300mg/day 52% ns • Placebo 48% All patients had supportive psychotherapy TADS
Cognitive and Social Skills Deficits in Adolescent MDD (1) • Prolonged difficulties with poor concentration, anhedonia and psychomotor retardation could affect intellectual development and academic achievement. • Attentional problems may interfere with processing of new, unfamiliar, or complex academic learning TADS
Cognitive and Social Skills Deficits in Adolescent MDD (2) • Social withdrawal and anhedonia interferes with normal social interactions with peers • This may appear as a failure to show proper initiative and reciprocity in interpersonal situations. • Irritability and non-verbal cues, such as poor eye contact, may discourage overtures and attention from peers and adults TADS
Goals of Cognitive-Behavioral Therapy (CBT) • Identification and modification of depressive thoughts and attributions • Increase participation in pleasant, mood enhancing activities • Increase and improve social interactions • Improve conflict resolution and social problem-solving skills • reduce physiological tension or affective arousal TADS
A Meta-Analysis of CBT Studies In Adolescent MDD(Reinecke et al, 1998) • 6 controlled studies meeting data criteria were examined, with 217 S’s, 10 comparisons • The overall post-TX Effect Size was (-)1.02, and F/U ES was (-).61 (F/U= 1-24 months) • Results suggested short-term and medium-term effectiveness for CBT TADS
Outcomes of CBT , Family and Supportive Therapy (Brent et al, 1997) CBT SBFT NST p-value Remission Rate 64.7% 37.9% 39.4% <.04 (BDI <9, 3 consecutive times) • CBT showed more rapid relief in interviewer (p< .03 and self-reported (p< .02) depression • All treatments showed significant and similar reductions in suicidality and functional impair-ment TADS
MDD and Suicide • The association between depression and suicidality in C/A is well-documented • 90% of attempters have a diagnosable disorder • Lethality of attempts and completed suicides increase in adolescence • Gender effects emerge after age 14, or in mid-adolescence TADS
Recurrence of MDD(Lewinsohn, Rohde, Klein, et al, 1999) • Follow-up of community sample at > 24 years old showed increase MDD (9.0% vs 5.6% vs 3.7% • 45% of adolescent MDD patients had recurrence (vs 18% in control group) TADS
Adult Outcome of Adolescent MDD (Brent et al, 1997; Weissman et al, 1998) • Early-onset MDD is associated with significant long-term impairment, including: • early parenthood • divorce • work and legal difficulties • substance abuse • suicidal behaviors TADS
This is a 5-year, NIMH-funded, multi-site effectiveness study of multi-modal interventions in 432 adolescents with MDD • 4 treatment-assignment arms are included: • fluoxetine (FLX) • cognitive-behavioral therapy (CBT) • combination fluoxetine and CBT (COMB) • pill placebo (PBO) TADS
NYU Medical Center Wayne State University New York, NY Detroit, NI Behavioral Health Center Southwestern Med. Center Charlotte, NC Dallas, TX University of Nebraska University of Chicago Omaha, NE Chicago, IL University of Oregon Johns Hopkins Hospital Eugene, OR Baltimore, MD Children’s Hospital of PA. NYS Psychiatric Institute Philadelphia, PA New York, NY TADS
The Carolinas Site (CHS)TADS Team Charles Casat, M.D. Jenny Kolker, Ph.D. Site PI, Pharmacotherapy Supervisor Site Co-PI, CBT Supervisor Marguerita Goldman, MS CBT Therapist and IE Michelle Perlmutter, N.P. Karyn Riedal, R.N. Independent Evaluator (IE) Nurse-Coordinator TADS
TADS Design (2)Treatment Stages • Stage I: 12 weeks of acute treatment (RCT) • Stage II: Consolidates gains for responders, and provides additional TX for partial responders • Stage III: To reduce risk of early relapse, this provides longer-term maintenance TX • Stage IV: 1-year follow-up to monitor for post-discontinuation relapse TADS
TADS Study Design Acute Consolidation Long-term Assess- Treatment Treatment Treatment ments (12 weeks) (6 weeks) (18 weeks) (1 year) Assess: 6 12 18 24 30 36 3 6 9 12 FLX X X X X CBT X X X X COMB X X X X PBO X 12-week COMB X PBO X X
TADS Inclusion Criteria • Age 12-17 inclusive • DSM-IV diagnosis of major depression • CDRS Depression Score > 45 • School grade placement 6th to 12th grade • Full-Scale IQ > 80 • Medication-free prior to start of study • Outpatient TADS
TADS Exclusion Criteria (1) • Bipolar Disorder, severe Conduct Disorder • Substance Abuse or dependence • Active suicidality, or homocidality • Thought disorder TADS
TADS Exclusion Criteria (2) • Failed 2 previous SSRI trials or CBT trial • Intolerance to fluoxetine • Concurrent therapy or medication • Non-English speaking patient or parent • No phone in home; Pregnant/breastfeeding TADS
Implications and Applications of TADS Findings • If drug TX is shown to have comparable efficacy and durability, there is considerable cost advantage in drug-only approaches • Conversely, if CBT or COMBO TX is shown to have greater efficacy and durability, there would be reason to recommend such a course because of long-term cost effectiveness, despite higher short-term costs TADS
Summary: MDD in Adolescents (1) • MDD can be diagnosed in C/A using unmodified DSM-IV criteria, except for irritability substituting for depressed mood • There is a familial aggregation of MDD, with early onset in children of depressed adults • MDD in this group significant comorbidity TADS
Summary: MDD in Adolescents (2) • Pediatricians, parents, teachers and are the early detectors of depression in adolescents • Negative developmental, academic and social outcomes, and risk for suicide • Vigorous and prolonged psychosocial and pharmacological interventions are indicated • The TADS is an NIMH program to study the best treatment(s) for depression TADS