Download
1 / 54
570 likes | 742 Views
Rehabilitation of Balance and Vestibular System Disorders. An introduction to the management of fall risk and vestibular patients. Arturo Miguel PT, MS, MBA. Introduction. Personal Background Why Balance and Vestibular Therapy?. Background.

E N D
Rehabilitation of Balance and Vestibular System Disorders An introduction to the management of fall risk and vestibular patients. Arturo Miguel PT, MS, MBA
Introduction • Personal Background • Why Balance and Vestibular Therapy?
Background • Falls are among the most common and serious problems facing elderly persons • Associated with considerable mortality, morbidity, reduced functioning, and premature nursing home admission • Generally result from an interaction of multiple and diverse risk factors, many of which can be corrected with education and physical therapy (Haddad, 2018)
Prevalence (CDC.gov) • Each year, 3 million older people who fall are treated in the emergency room • Risks usually become evident after injury • Additionally, falling is the leading cause of injury related death in seniors • Rate is three times higher in nursing homes and hospitals • Self imposed functional limitations • Recurrent falls are a common reason for admission to long term care institutions (40% of nursing home admissions)
Costs (CDC.gov) • Fall related injuries account for 6% of medical expenditures for persons over 65 • In 2015, the total medical costs for falls totaled more than $50 billion. Medicare and Medicaid shouldered 75% of these costs.
Course Objectives • Observe and identify deficits affecting balance senses and balance systems. • Demonstrate competence in performing balance and oculomotor screens. • Perform fall risk assessment and intervention plan. • Develop and execute evidence based treatment plans for patients with balance and/or vestibular dysfunctions including BPPV and vestibular weakness.
What is Balance? • The ability to maintain one’s center of gravity (COG) over a base of support (BOS) in a given sensory environment. • COG is at anterior to S2 in standing • BOS is your feet • Greater base laterally than A/P
Motor Response: Balance Strategies • Motor responses start from the ground up • Ankle Strategy • Hip Strategy • Stepping Strategy • Protective Reactions (Cheng, 2015)
Ankle Strategies • Primary strategy for balance • Controls sway
Hip strategies • Start when ankle strategies fail. Hips thrust anterior/posterior to shift COG over base of support.
What is normal sway? • In an everyday situation where there is minimal sensory inputs, we should rely on our ankle strategies. • A quick down and dirty way to observe sway is a Romberg and Sharpened Romberg Test.
Romberg Screen • Simple way to qualify and quantify patient’s standing balance • Have patient stand with feet close together, arms folded, for 20 seconds. • Observe patient for overall sway. • Watch for ankle, hip or stepping strategies. (Agrawall 2011)
Balance Strategies Video • Can you make any observations based on this patient’s balance strategies?
Balance Strategies Video #2 • Can you make any observations on this person’s balance strategies?
Stepping Strategies & Protective Reactions • If hip strategies fail, we take a step in the direction of the COG displacement in an attempt to increase our base of support. • If stepping strategies fail, we extend our upper extremities to protect from fall.
Other Strategies • “Squat Reactions” • Studies show when a posterior force is such that a person squats or attempts to flex knees in an effort to reduce the forces on spine. “Hopping Reactions” • Seen mostly in gymnasts when knee flexion is inhibited in response to a proper dismount. (Cheng, 2015)
Question • What diagnoses can you think of that may affect a person’s ankle Strategies? • Hip Strategies? • Stepping Strategies? • Protective Reactions?
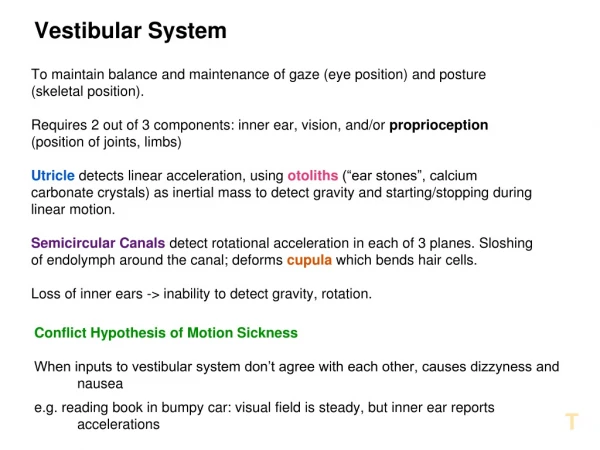
Balance Systems: Sensory • Three Balance Systems • Vision • Somatosensory • Vestibular
Visual System • Acuity/Sharpness vs. Oculomotor control • Acts as backup to somatosensory system (Tomamitsu, 2013) • Inputs may become more dependent with age. (Lee, 2017)
Somatosensory System • Feeling the ground under your feet • Includes sensation and proprioception in the joints • Acts as a backup to the visual system
Vestibular System • Senses angular rotation of your head as well as linear acceleration • Stabilizes vision via Vestibulo-Ocular Reflex (VOR) • Acts as a mediator when there is a conflict between the other two sensory systems.
Question • What diagnoses can you think of that may affect a person’s Somatosensory system? • Visual? • Vestibular?
Somatosensory System • Neuropathy (Tosizadeh, 2015 Camargo, 2015) • CVA (Hughes, 2011) • Ankle Injuries (Han, 2015) • MS (Fling, 2014) • LE Amputee (Hunter, 2017)
Visual System • Parkinson’s • Contrast sensitivity • Impaired visuospacial ability (Hill, 2016) • Multiple Sclerosis • Optic neuritis • Optic neuropathy (Hickman, 2014) • CVA • Visual field cuts • Visuospacial neglect (Winters, 2017)
Vestibular System • Vestibular hypofunction • A significant disparity between vestibular function from one side to the other (Iwasaki, 2015) • Meniere’s Disease • Presents with vertigo, pressure in the ear, tinnitus and profound sudden hearing loss(Nakashima, 2016) • Concussion • A mild TBI may result from blunt trauma to the head(Ayers, 2018)
Balance Screens • Romberg/Sharpened Romberg • 5 Times Sit to Stand • Timed Up and Go Test • Berg Balance Scale • Dynamic Gait Index • CTISB • Computerized Dynamic Posturography
5 Times Sit to Stand (5xSTS) • Equipment needed: Chair and stopwatch • Pt performs sit to stand five times without support • Timer starts when pt initiates sit to stand • Timer finishes upon sitting on 5th repetition • Normal times: <13.6 seconds (Guralnik, 2000) • Mean for Parkinson’s: 20.25 +/- 14.2 seconds (Duncan, 2011, Mong, 2010)
Timed Up and Go Test (TUG) • Equipment required: Chair, tape and stopwatch • Measure 10 feet from chair, mark with tape • Pt stands, ambulates 10 feet to marker, turns around and returns to sit in chair. • Timer starts upon standing then stops once pt is seated. • Normal time: • 60-69 years 8.1 seconds • 70-79 years 9.2 seconds • 80-99 years 11.2 seconds (Bohannan, 2006, Whitney, 2004)
Berg Balance Scale • Set of 14 functional tests • Patient is graded 0 to 4 points • Equipment required: • chair • ruler • stopwatch • stool or step • Normal score: >49 (Pereira, 2013) • Goal: Based on the score, up to 4 points in a 4 week period
Dynamic Gait Index (DGI) • Set of 8 functional gait tests • Equipment required: • stairs with rails • shoebox or step equivalent • 2 cones • stopwatch • Normal score: >19 (Whitney, 2004) • Goal: up to 3 point improvement in a 4 week period. (Johnson, 2011, Herman, 2009)
Observing Gait: A Review • Observe your patient the moment they stand up in the waiting room and walk towards the testing area. • Observe overall gait quality • Cadence • Decreased gait speed is associated with an increased mortality (White, 2013) • Decreased gait speed may also be consistent with fall risk (Roos, 2013) • Step length • Step width • Heel strike • Toe off • Arm swing
Common Gait Deviations • Antalgic • Ataxia • Spinal involvement (Gilbert 1978) • Cerebellar (Bultmann, 2014) • Shuffling • Parkinson’s (Rahman, 2008) • High Stepping/Foot slap or foot drop (Westhout, 2016) • Trendelenberg(Petrofsky, 2001) • Circumduction, Hip Hike (Burke, 2001)
Gait Deviations Video • What observations can you make on this person’s gait quality?
Gait Deviations Video #2 • What observations can you make on this patient’s gait quality?
Clinical Test for Sensory Integration and Balance (CTSIB) • Allows the tester to “isolate” balance systems with different conditions. • “Foam and Dome Test” requires • a foam cushion • a stopwatch • a lampshade-like dome (Whitney, 1998 Haghpeykar, 2003)
Computerized Dynamic Posturography • Utilizes force plate technology to qualify and quantify a subject’s use of balance senses as well as perform analysis on postural reactions. • Sensory Organization Test utilizes similar conditions as CTSIB • Considered “Gold standard” for sensory organization and postural testing (Alahmari, 2014)
Demo and Group Exercise • Separate into small groups • Practice each test with each other • 10-15 minutes for each group
Treatment Plan Considerations for the Non-Vestibular Balance Patient • Review the impairments and functional limitations • Consider activities that provide the most “bang for the buck” • Keep it simple • Be creative!
Examples of Balance Activities in Parallel Bars • Activity • Alternating Tap Ups/Cone Taps • Step-Ups • Lateral Step Ups • Step Up and Overs • Rationale • Promotes rhythmic weight shift, coordination and balance strategies (Roijezon, 2015)
Examples of Balance Activities in Parallel Bars • Activity • Ball Toss while on variable surfaces • Over the shoulder ball toss on variable surfaces • D1D2 Ball Handoff on variable surfaces with weighted ball • Rationale • Promotes coordination, ankle and hip strategies and A/P control • Promotes coordination and balance strategies and incorporates trunk and cervical rotation (Haran, 2008) • Adds strengthening to the above
Examples of Balance Activities • Activity • Tall kneeling activities • Activities sitting on a Theraball • Rationale • Helps to promote hip strategies and trunk stability
Examples of Balance Activities: Progression • Activity • Standing with head turns while on variable surfaces i.e. firm, foam, balance beam, dyna disc, tilt board • Rationale • Promotes sensory reweighting and balance strategies. • Head rotation stimulates vestibular function. • Variable surfaces promotes hip and ankle strategies.
Examples of Gait Activities • Activity • Gait with change speed slow/fast • Gait with gentle head turns • Sidestepping • Crossovers • D1D2Braiding • Rationale • Emphasizes improving gait quality • Head turns stimulates vestibular function with activity
Examples of Gait Activities: Progression • Activity • Gait with ball toss • Gait with lateral ball toss • Backwards walking • Rationale • Emphasizes improving gait quality, coordination and vestibular function