Download
1 / 29
310 likes | 378 Views
HIRSUTISM. Dr. Maysa’khadra MBBS, MMed(RHHG) A/P Reproductive Endocrinology and Infertility Jordan University Hospital. Introduction . Def: the presence of terminal ( coarse) hairs in females in a male-like pattern. It affects 5-15% of women

E N D
HIRSUTISM Dr. Maysa’khadra MBBS, MMed(RHHG) A/P Reproductive Endocrinology and Infertility Jordan University Hospital
Introduction • Def: the presence of terminal ( coarse) hairs in females in a male-like pattern. • It affects 5-15% of women • Usually associated with an underlying endocrine disoder : in 70-80% of women with hirsutism this is PCOS • Idioaapthic Hirsutim: isloated condition
Normal Hair Growth • 50 million hair follicle on the human body, 100,000-150,000 are found on the scalp • Palms, soles and lips are the only body parts lacking hair follicles • Few hair follicles form after birth • After the age of 40 years hair follicles decrease in number
Normal Hair Growth Three types of hairs: • Lanugo: a soft hair densely covering the fetus, usually shed in the 1st 4 months postpartum • Vellous: soft longer than lanugo hair (< 2cm), non pigmented which covers the body • Terminal longer, pigmented , makes up the yebrows, scalp and axillary and pubic areas
Normal Hair Growth • Three phases of hair growth: • anagen: active growing phase • catagen: involuting phase : when the hair stops growing • telogen resting phase , when the hair is shed • There is disharmony in the phases of hair growth ; thus while some hairs are in the anagen , others are resting • The overall length of the hair is determined by the duration of the anagen phase
Regulation of Hair Growth • Multifactorial; local and systemic factors and sex hormones act on dermal papillae to promote hair growth • Deficiences in thyroid and growth hormone alter anage; telogen ratio in scalp and body hair • testosterone 5-αreductaseDihydrotesterone in the hair follicle • Andostenedione and Dehydroepiandrosterone are metabolized in the skin to Testosterone and DHT
Regulation of Hair Growth • Sensitivity of hair follicles to androgens varies over the body. • Hair growth in the eyelashes, eyebrows and the occipital and lateral aspects of the scalp is mostly independent of androgenic effects • axillae and pubic areas are sensitive to low levels of androgens • Chest, lower abdomen, face, upper thighs and lower back need high levels of androgens to increase hair growth. Thus when hairs are found in these areas they are described as ‘male pattern’ and considered pathological in women
Aetiology • Androgen Excess: • PCOS • Androgen secreting tumors • Non classical congenital adrenal Hyperplasia • Other causes • Non androgenic factors • Idiopathic factors
Polycystic Ovary Syndrome • Most common cause of hirsutism, 70-80% of cases • Diagnosis based on the revised criteria adopted in Rotterdam 2004: 2 out of 3 are enough for the diagnosis after the exclusion of other causes: • oligo- or anovulation • clinical or biochemical hyperandrogenism • Morphological features of polycystic ovaries on Ultrasound scan
PCOS and IR • Insulin resistance is important in the etiology • Insulin increases androgen levels by increasing androgen production by the ovarian theca cells and indirectly by reducing hepatic synthesis of SHBG. • 30-75% of women with PCOS are overweight, which increases insulin resistance and exacerbates hyperandrogenaemia.
Androgen secreting tumors • Ovarian or adrenal • they are rare , between 1 in 300 and 1000 • suspect if onset is rapid, or if they lead to virilisation or they are associated with cushingoid features. • Diagnosis is best by clinical presentation • ovarian tumours associated with androgen excess : arrenoblastomas; Leydig, hilar and thecal cell tumours; and luteomas of pregnancy • >50% of adrenal tumors associated with hirsutism are malignant
Non classical congenital adrenal Hyperplasia • AR • 1.5-2.5% of hisute women • 21- hydroxylase ceficiency resulting in high 17-OH progesterone, which is androgenic
Other causes • Thyroid dysfunction • Acromegaly • Cushing syndrome • Hyperprolactinemia • women with these conditions present with symptoms other than hirsutism
HAIRAN • Hyperandrogenic insulin-resistant acanthosis nigricans syndrome is an inherited condition that occurs in 3% of women with hirsutism • Extremely high levels of insulin due to severe insulin resitance • Women are severly hyperandrogenic • Very difficult to treat • they can cause virilization
Androgenic drugs • Testosterone, Danazol and anabolic steroids all induce hirsutism via their inherent androgenic prosperities
Non-androgenic factors • unknown mechanism on hair follicle independent of androgens • Drugs: • Phenytoin • Minoxidil • Diazoxide • Psoralen • Pencillamine
Idiopathic Hirsutism • all other causes are excluded • normal menses • normal ovarian appearance • No detectable hormonal abnormalities • No evidence of adrenal or ovarian tumors • prevalence is less now with more diagnostic techniques (6-7%)
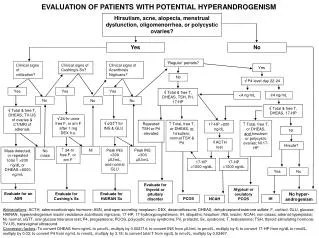
Evaluation • In depth History Drugs, changes in weight or facial contour, presence of acne, hair loss/balding, menstrual and reproductive history and relevant family history , such as premature male balding and diabetes in the context of PCOS • Physical Exam: extent, type and pattern of hair growth, signs of virilisation , thyroid enlargement, galactorrhea, pelvic / abdominal masses, cushingoid features, obesity and signs of systemic illness
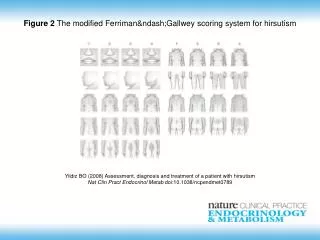
Ferriman and Gallwey (1961) scoring system • They scored the density of hair at 11 different body sites; namely the upper lip, chin, chest, upper back, lower back, upper abdomen, lower abdomen, arm, forearm, thigh, and lower leg • 0: absence of terminal hair,4: extensive terminal hair growth,Scores > 6 were deemed significant • Hatch et al 1981 modified scheme (9 sites) excluding lower legs and forearms as these are less sensitive to androgens • These schemes are typically used for research rather than clinical setting
Evaluation • Mild hirsutism ( FG 8-15) without any other features such as menstrual irregularities can be treated cosmetically and investigated further if treatment fails or hirsutism worsens • Moderate- severe hirsutism ( FG > 15), it is likely that androgen excess is present , the possible causes should be investigated. History and examination would dictate which investigations are appropriate
Investigations • Free testosterone levels are the most sensitive measure of hyperandrogenism • A very high ( > 1.5-2 ng/ml) testosterone level increases the likelihood of neoplasm • Increased DHEA-S indicates an adrenal source • Non- classical congenital adrenal hyperplasia; increased testosterone and 17-OH progesterone > 200ng/dl ( can be slightly elevated in PCOS). • Pelvic US can help in the diagnosis of PCOS or ovarian tumors though can be normal in both of these conditions.
Management • Lifestyle changes, cosmetic , physical and hormonal therapies • Cosmetic and hormonal therapies are effective as long as they are in place, more permanent reductions cab be achieved using physical methods
Life style changes and weight reduction • Weight loss reduce hyperandrogenism and insulin resistance , esp. in overweight women with PCOS • Weight reduction of 5-10% can improve hirsutism by 40-55% within 6 months of weight loss • In obese women with PCOS, weight loss programmes should be first line of intervention, to include low calorie diet and exercise over 6 months
Cosmetic methods • Plucking, waxing, bleaching, the use of depilatory creams. • shaving should be avoided as it leads to blunt hairs that may feel like stubble- although no increase in hair growth which is a misconception. • Depilatory and creams decrease local hair but chronic use can cause skin irritation • plucking and waxing can cause folliculitis and ingrown hairs in androgenic areas
Physical • Electrolysis: expensive, time consuming (18 months to 4 years), painful and really practical for a limited area. It may cause depigmentation and scarring. • Laser photothermolysis:used to destroy hair follicles without damaging nearby tissue. It can cover a wider area than electrolysis. It is best for fair skin women. It reduces hair density by 30% after 3-4 sessions
Hormonal therapy • The basis of action is either the suppression of androgen production or blocking of the action of androgens on the skin. • This results in the hairs reverting back to vellus-type hair. • it takes 9-12 months for the maximum effects to be noticed. Can be combined with cosmetic measures.
Hormonal therapy • Combined oral contraceptive pill • Cyproterone acetate • Spironolactone • Finesteride • Flutamide • Insulin sensitizers: metformin • Cell cycle inhibitors: Eflornithine • Gonadotrophin-releasing hormone agonists