Download

1 / 59
740 likes | 1.31k Views
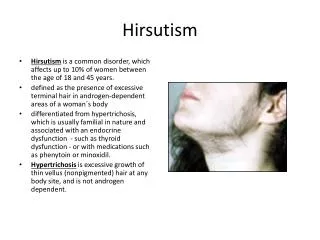
Approach to Hirsutism. Hemmatabadi M., MD Assistant professor of Tehran Medical University. Definition. Lanugo : in infants, androgen-independent hair, soft vellus unpigmented hair that covers the entire body .

E N D
Approach to Hirsutism Hemmatabadi M., MD Assistant professor of Tehran Medical University
Definition • Lanugo: in infants, androgen-independent hair, soft vellusunpigmented hair that covers the entire body. • Hypertrichosis : diffusely increased total body hair, rare, usually caused by a drug ( phenytoin, dexamethasone, diazoxide, minoxidil, and cyclosporine) or systemic illnesses ( hypothyroidism, anorexia nervosa, malnutrition, porphyria, dermatomyositis, & as aparaneoplastic syndrome ) • Hirsutism : androgen-dependent terminal body hair ( stiff, pigmented ) in a woman in places in which terminal hair is normally not found (face, chest, abdomen, back ).
Epidemiology • overall prevalence of hirsutism is unknown. • The definition of normal must also consider race & ethnicity Most Asian & Native American women have little body hair, while Mediterranean women on average have moderately heavy body hair; serum androgen concentrations are similar in the three groups • The most important consideration, whatever the woman's background, is whether the pattern of hair growth has changed or the rate of growth has increased.
Etiology • ↑androgen production (by the ovaries or adrenal) • ↑Testosterone is usually of ovarian origin • ↑Dehydroepiandrosterone sulfate (DHEA-S) is of adrenal origin • ↑Androstenedione can be of either adrenal or ovarian origin • Rarely ↑ target organ production of androgen
Idiopathic hirsutism • women with hirsutism and no other clinical abnormalities ( Nl ovulatory function , and no identifiable cause of their hirsutism ). • Ovulatory function may be verified by a luteal phase day 7 progesterone, which should be at least 5 ng/ml. • Total & free serum testosterone are more often within the normal range. • More in women of Mediterranean ancestry. • There may be↑cutaneous 5-- reductase activity.
Polycystic Ovary Syndrome • The most common identifiable cause of androgen excess in women • The minimum criteria for this diagnosis are : • Menstrual irregularity, due to oligo- or anovulation • Evidence of hyperandrogenism, whether clinical (hirsutism, acne, or male pattern balding) or biochemical (elevated serum androgen concentrations) • Exclusion of other disorders such as congenital adrenal hyperplasia and androgen-secreting tumors.
Polycystic Ovary Syndrome • the diagnosis does not require biochemical tests (except as needed to R/O other disorders) or pelvic US to evaluate ovarian structure. • Usually becomes evident about the time of puberty or soon thereafter. • the symptoms gradually worsen with age.
DDx. of PCOS • Idiopatic hirsutism • Hyperprolactinemia • Hypothyroidism • Nonclassical CAH • Ovarian tumors • Adrenal tumors • Cushing’s syndrome • Glucocorticoid resistance
Hyperprolactinemia • Some women with hirsutism have mild hyperprolactinemia, but whether it alone can cause hirsutism is not clear. • Sometimes associated with ↑ serum DHEA-S concentrations (prolactin receptors have been identified in human adrenal cells, and prolactin can increase adrenal DHEA secretion)
Hyperprolactinemia • Underlying problem in many of these women is probably the PCOS. • DHEA-S is such a weak androgen that the hirsutism associated with hyperprolactinemia is probably due more to the ovarian hyperandrogenism characteristic of the PCOS than any effect of hyperprolactinemia.
CAH • Basal (8 AM) 17OHP > 8 ng/ml is diagnostic. 2-8 ng/ml ( CAH or PCOS ) A rise at least 10 ng/ml 60 min. after IV ACTH is diagnostic for nonclassical CAH.
Hyperthecosis • Nonmalignant ovarian disorder • ↑ production of testosterone by luteinized thecal cells in the stroma. • It is still unclear if hyperthecosis is a distinct disorder or is part of the spectrum of the PCO. • The woman's history usually is one of gradual onset of hirsutism and other manifestations of androgen excess.
Ovarian Tumors • Occur later in life and progress more rapidly • Androgen-secreting tumors constitute only 5 percent of all ovarian tumors • Histologically : Sertoli-Leydig cell tumors(androblastoma, arrhenoblastoma), granulosa-theca cell(stromal cell) tumors, and hilus-celltumors. • Serum testosterone ≥ 1.5 - 2.0 ng/ml ( ×3 the upper limit of Nl in women is 0.60 to 0.80 ng/ml) • Many of these tumors can be identified by vaginal US.
Adrenal Tumors • Rare cause of androgen excess • Most are carcinomas that often secrete not only androgen ( mostly DHEA and DHEA-S ) • May lose the ability to sulfate DHEA Nl serum DHEA-S value does not exclude the Dx. • An unequivocally elevated serum DHEA-S ( >700 μg/dl ) is suggestive of an adrenal tumors.
Insulin Resistance • Possibly acting via the theca-cell receptors for IGF-1 • Insulin also ↓ serum SHBG ↑ fraction of serum testosterone that is free at any serum total testosterone concentration.
Diagnostic Approach • Documentation of the degree of androgen excess • Exclusion of the serious but rare causes of hirsutism such as hyperprolactinemia due to pituitary and hypothalamic tumors and ovarian and adrenal tumors
findings that suggest one of the rare causes of hirsutism • Abrupt onset, short duration (typically < 1 year), or progressive worsening of hirsutism. • Onset in the 3rd decade or later, rather than near puberty. • Symptoms or signs of virilization ( frontal balding, acne, clitoromegaly, increased muscle mass, or deepening of voice). More severe hirsutism and virilization are typically seen in ovarian hyperthecosis. • Moderately elevated serum androgen concentrations : serum testosterone > 150 ng/dL, serum free testosterone > 2 ng/dL, and serum DHEA-S >700 µg/dL in young♀.
The important elements of the history • The age of onset of hirsutism, its nature (vellusvs. terminal), and the rate of progression • The benign forms of hirsutism [hyperthecosis, nonclassical congenital adrenal hyperplasia (CAH), and obesity related insulin resistance] tend to begin in the pubertal years • Hirsutism that appears clearly before puberty or clearly after puberty is more often caused by an ovarian or adrenal neoplasm, or it is medication related
History Menstrual history • The normal menstrual pattern varies with age. In pubertal girls, the average cycle length is 34 d. In older women, it is 28 d. • A normal pattern is roughly 12 cycles per year, varying in length, the longest cycle minus the shortest cycle being no more than 10 d - Women with consistently regular cycles and symptoms of ovulation are unlikely to have severe hyperandrogenemia. - A woman who has irregular cycles should be evaluated for hyperprolactinemia.
History • Cutaneous manifestations of hyperandrogenism - frontal balding - acne • Time course of symptoms : progressive worsening of hirsutism, a later age of onset, or rapid rate of progression suggest the possibility of ovarian or adrenal tumor • Weight history : Obese women have increased androgen production • Medication history: drug Hx. ( danazol, norgestrel )
History • Family history - Hirsutism, acne, menstrual irregularity, infertility, early cardiovascular disease, and obesity are all potential indicators of a familial tendency towards the PCOS. - A family history of known or suspected CAH would prompt a ACTH stimulation test.
Physical Examination • Body habitus – The pattern of body fat distribution (truncal obesity, a buffalo hump, and supraclavicular fat) may suggest the presence of Cushing's syndrome. • Skin – The location and quantity of terminal hair should be determined objectively using the Ferriman-Gallwey score. A total score > 8 is considered to be abn. Acne, seborrhea, temporal balding, acanthosis nigricans ( suggest insulin resistance), striae, thin skin, or bruising (suggest Cushing's syndrome )
Physical Examination • The male terminal hair pattern differs from the female pattern with temporal balding, full beard distribution, hair over the shoulders, chest, and upper abdomen. • The female terminal hair pattern lacks temporal balding and terminal facial hair other than on the upper lip and chin. • Normal women have no terminal hair on the shoulders and chest other than a few periareolar hairs. It is very uncommon for women to have terminal hair on the upper abdomen
Physical Examination • Signs of virilization – In addition to acne, deepening of the voice, frontal (or crown) balding, increased muscle mass, and clitoromegaly [clitoral length >10 mm or the clitoral index ( length × width ) >35 mm2 ] indicate the presence of moderate androgen excess.
Physical Examination • Galactorrhea – The presence of any breast discharge (spontaneous or expressible) is suggestive of hyperprolactinemia and warrants measurement of serum prolactin even if the woman's menstrual cycles are regular. • Abdominal and pelvic examination – may reveal mass lesions that could indicate the presence of an androgen-secreting tumor.
Laboratory Testing • Serum Testosterone - the best overall estimate of androgen production in hirsute women is the single best test - values < 150 ng/dL (5.2 nmol/L) exclude ovarian or adrenal tumors, also tend to exclude ovarian hyperthecosis. - most women with the PCOS have serum testosterone < 150 ng/dL & are sometimes normal; women with idiopathic hirsutism are even more likely to have normal values.
Serum Testosterone In all women with androgen excess ( PCOS, hyperinsulinemia, idiopathic hirsutism ) serum free testosterone concentrations are disproportionately higher than serum total testosterone concentrations. Androgen excess ↓ hepatic production of SHBG
Laboratory Testing • Serum Prolactin : -If ↑serum testosterone in an anovulatory woman serum TSH & prolactin to R/O anovulation associated with hyperprolactinemia moderately elevated value should be followed by imaging of the hypothalamic-pituitary region. - slightly elevated values can be found in women with PCOS.
Laboratory Testing • Serum DHEAS - should be measured in women with rapidly progressing hirsutism and in those who are virilized. - Nl or slightly increased in most ♀ with androgen excess. - values > 700 µg/dL (13.6 µmol/L) in a young woman, suggest the presence of an adrenal tumor. - secretion of DHEA-S begins to fall after age 20 years serum DHEA-S must be interpreted according to age-specific normal ranges. - Low values have been reported in a few women with adrenal carcinoma, however, due to lack of sulfating activity within the tumor.
Summery • Women with long-standing mild hirsutism, not different from family members, and regular ovulatory menstrual cycles require no laboratory testing at all. • The Endocrine Society guidelines suggest testing in women with moderate to severe hirsutism, or for hirsutism associated with irregular menses, obesity, signs of virilization, or rapid progression
Summery • Women with mild to moderate hirsutism should have measurements of serum testosterone; serum prolactin & TSH should also be measured if menstrual cycles are irregular. • Serum DHEA-S should be measured in addition to testosterone in women with progressive hirsutism, irregular menstrual cycles, and any signs of virilization
Additional test in selected patient • Serum FSH - if there is any suspicion of declining ovarian estrogen production ( periods of amenorrhea or menopausal symptoms ). - Serum FSH should be elevated if estrogen production is reduced. - Low estrogen production can contribute to increased hair growth by reducing SHBG production, thereby raising serum free testosterone.
Additional test in selected patient • Serum LH - Women with PCOS tend to have elevated serum LH concentrations and normal or low serum FSH. - high LH/FSH ratio is not required for the diagnosis, because LH secretion is pulsatile and many women with PCOS have normal serum LH concentrations-because the LH measurement was obtained at the nadir of a pulse.
Additional test in selected patient • Pelvic Ultrasonography To screen for ovarian tumors - Suspicious findings include large cysts, solid masses, and complex cysts that do not resolve spontaneously in 2-4 wks. - The sensitivity and specificity of US for the Dx. of ovarian tumors in hyperandrogenic women has not been determined. - Small hilus-cell tumors of the ovary that produce large amounts of testosterone may not be seen by US or even at the time of surgery.
Pelvic Ultrasonography can also be used to identify polycystic ovaries - enlarged ovaries, consist of a ring of small peripheral follicles, typically each < 8 mm, with an increased amount of central stroma. - However, the correlation between polycystic ovaries, as detected by US & the PCOS is only fair. -women with non-ovarian causes of hirsutism, such as CAH and adrenal tumors, may have polycystic-appearing ovaries.
Pelvic Ultrasonography Indications • In patients with an elevated serum androgen concentration if a tumor is suspected. • It may also be indicated to exclude endometrial hyperplasia, which is common in PCOS.
Additional test in selected patient • Testing for CAH - should be considered in women with an early onset of hirsutism (including those with premature adrenarche), hyperkalemia , a F Hx. of CAH, or a strong desire to know a specific etiologic diagnosis. -by measuring serum 17-hydroxyprogesterone (and cortisol) before and 60 min. after IV injection of 250 µg of synthetic ACTH (cosyntropyn, ACTH amino acids 1-24) A positive test consists of a 60-minute serum 17-OHP value > 10 ng/mL (30 nmol/L).
Additional test in selected patient • Testing for Cushing’s Syndrome - if hirsute women have symptoms and signs of cortisol excess, screening for this disorder may be indicated. - by measuring 24-hour urinary excretion of cortisol (and creatinine) or by performing an overnight DST.
Additional test in selected patient • Abdominal CT or MRI - Is indicated to look for an adrenal mass if the woman has a markedly elevated serum DHEA-S concentration or other evidence of excess adrenal steroid production. • Radiologic testing is otherwise not indicated, and may be misleading, because nonfunctioning adrenal masses are common
Additional test in selected patient • Laparascopy or Laparatomy - In a hirsute woman who has menstrual abnormalities, a serum testosterone > 200 ng/dL (6.9 nmol/L), and no evidence of an adrenal tumor. - Such a patient may have a small ovarian tumor (especially a hilus-cell tumor) that is too small to be detected by pelvic ultrasonography.
Summery • Endocrine Society suggest measuring serum total testosterone and DHEA-S in all women presenting with hirsutism. • We suggest an adrenal CT scan to look for an adrenal androgen-secreting tumor if the serum DHEA-S concentration is ≥700 mcg/dL • We suggest a transvaginal ultrasound if the serum total testosterone concentration is ≥150 ng/dL