Download
1 / 35
350 likes | 374 Views
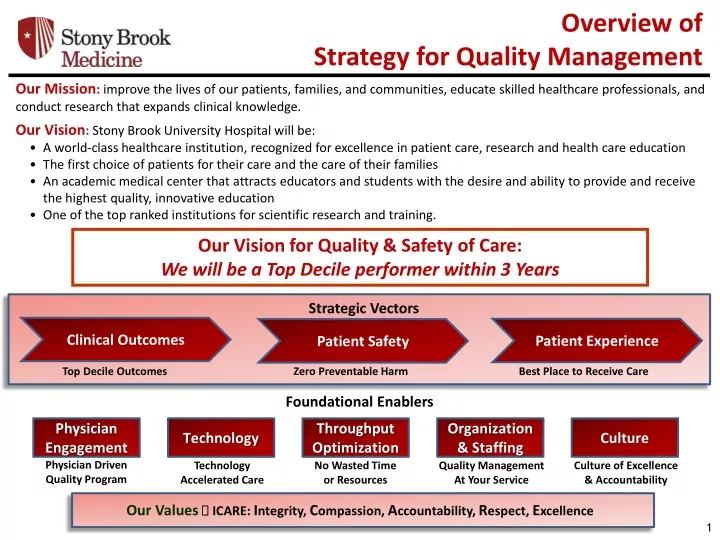
Overview of Strategy for Quality Management. Our Mission : improve the lives of our patients, families, and communities, educate skilled healthcare professionals, and conduct research that expands clinical knowledge. Our Vision : Stony Brook University Hospital will be:

E N D
Overview of Strategy for Quality Management Our Mission:improve the lives of our patients, families, and communities, educate skilled healthcare professionals, and conduct research that expands clinical knowledge. Our Vision: Stony Brook University Hospital will be: • A world-class healthcare institution, recognized for excellence in patient care, research and health care education • The first choice of patients for their care and the care of their families • An academic medical center that attracts educators and students with the desire and ability to provide and receive the highest quality, innovative education • One of the top ranked institutions for scientific research and training. Our Vision for Quality & Safety of Care: We will be a Top Decile performer within 3 Years Strategic Vectors Clinical Outcomes Patient Experience Patient Safety Top Decile Outcomes Zero Preventable Harm Best Place to Receive Care Foundational Enablers Physician Engagement Technology Throughput Optimization Organization & Staffing Culture Our Values ICARE: Integrity, Compassion, Accountability, Respect, Excellence Physician Driven Quality Program Technology Accelerated Care No Wasted Time or Resources Quality Management At Your Service Culture of Excellence & Accountability
Early Detection and Treatment of Severe Sepsis and Septic Shock Stony Brook University Medical Center April 2017
Surviving Sepsis and Septic Shock Mortality rates associated with sepsis • 30-50% for severe sepsis • 50-60% for septic shock Severe sepsis is the leading cause of death in the non-coronary ICU Sepsis kills approximately 1,400 people worldwide every day
Severe Sepsis Recommendations Adult and Pediatric Evidence-based Studies • Early Detection • Early Treatment • Sepsis Resuscitation Bundle • 3. Monitor reliability and outcomes
New York State Department of Health (NYSDOH) Reporting • Effective May 1, 2013 NYSDOH Title 10 New York Codes Rules and Regulations (NYCRR) Sections 405.2 and 405.4 were amended to require that hospitals have in place evidence-based protocols for the early recognition and treatment of patients with severe sepsis and septic shock that are based on generally accepted standards of care. Population • Inpatient adults (>18 y/o) and children (≤18 y/o). • Diagnoses of Severe Sepsis or Septic Shock
Center for Medicare and Medicaid Services (CMS) Reporting CMS Core Measure (SEP-1) Population Inpatients age 18 and over Diagnosis of Sepsis, Severe Sepsis, or Septic Shock
Why This Is Important • Adherence to protocol guidelines will improve patient mortality outcomes! • Hospital Inpatient Quality Reporting is ‘Pay for Performance’ • Stony Brook mustparticipate in all mandatory Inpatient Quality Reporting Measures • Public Reporting of CMS and NYSDOH data
Defining The Septic Picture • SIRS (Systemic inflammatory response syndrome): The clinical syndrome that results from a deregulated inflammatory response or to a noninfectious insult. • Sepsis:SIRS that is secondary to infection that has been diagnosed clinically. Positive cultures add to the validity but are not required for the diagnosis. • Severe Sepsis: Sepsis plus at least one of the signs of hypoperfusion or organ dysfunction that is new, and not explained by other known etiology of organ dysfunction. • Septic Shock: Severe sepsis associated with refractory hypotension (BP<90/60) despite adequate fluid resuscitation and/or a serum lactate level >=4.0 mmol/L.
Adult Severe Sepsis CriteriaAll three of the following must be met within 6 hours of each other. • Documentation of a suspected source of clinical infection • B. Two or more manifestations of systemic infection according to the SIRS criteria, which are: • Temperature > 38.3 C/101 F or < 36.0 C/96.8 F • Heart rate > 90 bpm • Respiration > 20 per min • WBC > 12,000 or < 4,000 (k/uL) or > 10% bands • C. Organ dysfunction, evidenced by any one of the following: • SBP < 90 (mmHg), or MAP < 65 (mmHg), or a SBP decrease of more than 40 pts (if documented by LIP as due to infection) • Cr > 2.0 (mg/dL), or urine output < 0.5 mL/kg/hour for 2 hours • Bilirubin > 2 mg/dL (34.2 mmol/L) • Platelet count < 100,000 (k/uL) • INR > 1.5 or a PTT > 60 sec • Lactate > 2 mmol/L (18.0 mg/dL) • Acute respiratory failure requiring a new need for invasive or non-invasive mechanical ventilation • OR Physician/NP/PA documentation of severe sepsis
Septic Shock Criteria • Patient meets Severe Sepsis criteria ANDeither: • Lactic acid ≥4 mmol/L OR • Persistent Hypotension in the hour following crystalloid fluid bolus OR • Physician/Advanced Practitioner diagnosis
Lactate Collection Blood culture collection prior to broad spectrum antibiotics Early and appropriate broad-spectrum antibiotic administration Interventions within 3 Hours of Recognition
Reminder! • Blood cultures must be collected prior to antibiotic administration time. Check that the collection time is correct on all blood culture orders before sending to the lab • Nurses may override the Pyxis for certain antibiotics, become familiar with those available in your area • Timely antibiotic administration is a priority in the treatment of sepsis!!
Fluid Resuscitation • Crystalloid fluid resuscitation (30 ml/kg) must be initiated within 3 hours of: • Septic shock presentation • Crystalloid fluid resuscitation (30 ml/kg) must be completed within 6 hours of: • Septic shock, by diagnosis or clinical criteria OR • Lactic Acid ≥4 mmol OR • Any episode of hypotension (SBP <90 or MAP<65 mmHg) within 6 hours following severe sepsis presentation time.
Re-measure lactate if the initial value was elevated (>2.0 mmol/L) Interventions within 6 Hours of Recognition Cerner Lactate Re-Order Rule Screens lactate results >= 2.1 for Inpatient, Emergency and Observation patients The system generates another Lactic Acid with the start of current time + 4 hours, with a frequency of 2 times If the first result of the first system generated order comes back <2.1 the second system order is discontinued
Vasopressor therapy for persistent hypotension (MAP <65 mmHg in adults) IF hypotension persists after fluid administration Includes a repeat volume status and tissue perfusion assessment within 6 hours of presentation of Septic Shock Interventions within 6 Hours of Recognition contd.
Volume Status and Tissue Perfusion Assessment A focused exam performed/reviewed by physician/advanced practitioner must be documented, including: Vital Signs Cardiopulmonary Capillary refill Peripheral pulses Skin
Refusal of care must be specifically documented within 6 hours of the presentation of severe sepsis or septic shock for: • Antibiotics • Blood Draws • IV Fluids • Vasopressors • Comfort Measures or Palliative Care • Within 3 hours of the presentation of severe sepsis • Within 6 hours of the presentation of septic shock Bundle Variance Documentation
Pediatric Severe Sepsis Criteria • Sepsis plus one of the following: • Cardiovascular Organ Dysfunction • OR • Acute Respiratory Distress Syndrome • OR • Two or more other organ dysfunctions Pediatric Septic Shock Criteria Pediatric Organ Dysfunction Criteria Cardiovascular Respiratory Neurologic Renal Hepatic Sepsis and cardiovascular organ dysfunction
Recognition to Immediate Treatment The Pediatric Acute Sepsis Multiphase Power plan Early Detection and Treatment of Severe Sepsis
Cerner Sepsis Screening Alert • 2 SIRS criteria within a 5hr period will trigger a task to fire in Cerner for the bedside nurse to evaluate their patient for suspicion of infection. • If an infection is suspected, the RN contacts the physician for a sepsis workup. The RN documents name of physician and date/time notified. If the nurse answers “yes” to a suspicion of infection, a lactate is ordered via option on the admission power plan. The Adult and Pediatric Sepsis Multiphase Power plans are offered under suggested power plans. • If the screen is found to be negative, complete the task as “No.” Comments should be entered, the section should not be left incomplete • Once addressed, the alert will not fire again for an 8 hour period.
The Pediatric Amendment • Applying the alert to our pediatric population required creation of seven additional “rules” for age specific criteria. • Power plan prompts • Duration adjustments in the ED
Sepsis Alert Recognition-Nursing • Mandatory fields answered by the RN, including notification and comments regarding their decision. • Physician notification • Generates serum lactate draws based on Admission Power Plan orders. • Includes suggestions of Sepsis Power plan use for treatment.
Cerner Severe Sepsis Screening Alert • This alert will appear whenever a physician opens the patient’s chart and the following criteria have been met: • 2 SIRS criteria + 1 Organ Dysfunction (within 6 hours of each other) • The alert will ask the provider to agree or disagree with severe sepsis or allow documentation of comfort measure initiation or refusal of treatment.
Severe Sepsis Recognition Provider • If the provider agrees, , the alert generates an order stating severe sepsis is present. • If criteria are not already met, this would be the Protocol Initiation Time and all elements of the bundles must be completed within 3 and 6 hours respectively. • If the provider disagrees, the alert will desist for 12 hours and an order will be generated documenting the patient does not have severe sepsis. • If the patient or family has refused treatment or comfort measures are initiated, a form will open to document and a clinical note will be generated.
Comfort Measures/Refusal of Treatment This form opens to allow you to document the discussion or initiation of comfort care and refusal of treatment
Severe SepsisDocumentation Clinical Notes – Comfort Measures/Refusal of Treatment Note Generated Orders- Severe Sepsis Present Order is generated with Physician Name, Date, and Time
Cerner Septic Shock ScreeningAlert • If the provider has “agreed” to the severe sepsis alert, the Septic Shock Alert will look for: • Lactic acid >4 mmol/L with 6 hours • If criteria is found the alert will fire, notifying the provider of potential septic shock.
Septic Shock Alert Documentation • If the provider agrees with the alert, he/she will be prompted to complete a focused exam. An order is generated stating Septic Shock is Present. • If the provider disagrees, an order will be generated stating septic shock is not present.
SepticShock Alert Form • The boxes auto fill with data last charted, i.e. vital signs and elements for review, which will include documentation from Iview. • The provider will click on the green check mark to complete the form. Boxes
Septic Shock- Chart Documentation Clinical Notes Orders- this order will appear when the provider has clicked “disagree with septic shock”
In Summary… • Early recognition is essential • Lactate is an early predictor of organ dysfunction • Early fluid resuscitation and administration of antibiotics is critical • Sepsis Powerplans and Caresets are available and up-to-date
References Dellinger, R. Phillip et al, Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Critical Care Medicine, Feb. 2013. Vol. 41, No.2. Goldstein, Brahm, et al, International Pediatrics Sepsis Consensus Conference: Definitions for sepsis and organ dysfunction in Pediatrics. Pediatric Critical Care Medicine, 2005, Vol.6 No. 1. Surviving Sepsis Campaign: An international collaborative recommending resuscitation and management care bundles for the recognition and treatment of sepsis/septic shock. Recommendations were first published as in Critical Care Medicine, Mar 2004. Link to Policy