Download
1 / 40
470 likes | 776 Views
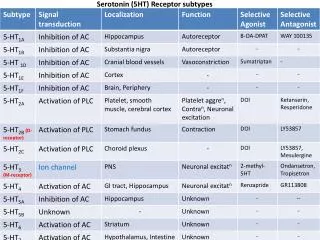
Lecture 5 - Serotonin. The serotonergic neuron. Serotonin. serotonin = 5-HT (5-hydroxytryptamine) an ‘indoleamine’ – has an indole ring structure this structure is also found in ‘hallucinogenic’ or ‘psychedelic’ drugs. Indole ring structure. Serotonergic systems. Serotonergic systems.

E N D
Serotonin • serotonin = 5-HT (5-hydroxytryptamine) • an ‘indoleamine’ – has an indole ring structure • this structure is also found in ‘hallucinogenic’ or ‘psychedelic’ drugs
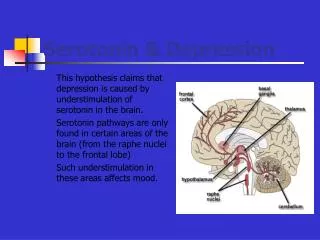
Serotonergic systems • the major serotonergic systems originate in the raphe nuclei (in the brain stem) and project to areas throughout the brain • these projections appear to have a primarily inhibitory function, acting in opposition to cholinergic, noradrenergic & dopaminergic projections
Serotonergic systems • increased serotonergic activity is associated with reduced levels of behavioural activation & arousal • serotonin plays an important role in sleep, mood, appetite, temperature regulation & pain perception
Serotonin & cognition • effects of manipulating serotonin are highly task-dependent • increasing or decreasing serotonergic activity can improve or impair cognitive performance (or have no effect), depending on nature of task
tryptophan hydroxylase 5-HTP decarboxylase 5-HT 5-HTP Serotonin (5-HT) synthesis tryptophan
Acute tryptophan depletion (ATD) • ATD is used in experimental studies to reduce levels of 5-HT in the brain • subjects ingest a drink containing a concentrated mixture of amino acids, but notryptophan • this induces protein synthesis (which requires tryptophan) • therefore, available tryptophan in the body is used up • this results in a decline in 5-HT synthesis in the brain
Increasing serotonergic activity • tryptophan supplementation • buspirone - a ‘mood enhancer’ used to treat anxiety & depression • SSRI antidepressants – e.g. fluoxetine (= Prozac), paroxetine (= Seroxat) • ‘psychedelic’ drugs - LSD, mescaline (peyote), psilocybin (‘magic’ mushrooms), MDMA (‘ecstasy’)
Serotonin & mood • ATD is associated with negative mood in normal subjects – e.g. increased irritability & aggressiveness • ATD can cause a temporary recurrence of depressive symptoms in some subjects (~50%) who have a history of depression • see Young & Leyton (2002)
Serotonin & mood • increasing serotonergic activity through tryptophan supplements, direct 5-HT agonists (e.g. buspirone), or selective serotonin reuptake inhibitors (SSRIs) is associated with more positive subjective mood reports in both ‘normal’ subjects and those with a history of mood disorders
Buspirone – effects in normal subjects Effect of buspirone on self-report ‘contentedness’ after 2 hrs cognitive performance testing (drug had no significant effect on any performance measure) – Chamberlain et al (2007) Journal of Psychopharmacology 21, 210-215
Depression • intense feelings of persistent sadness, helplessness & hopelessness • inability to experience pleasure in activities that are normally pleasurable (anhedonia) • tiredness & lack of energy • abnormal sleep & eating patterns (increased or decreased) • cognitive impairments – difficulty concentrating, deficits in memory & executive functions • affects 10-20% of people at some point in their lifetimes • website: www.DepressionAlliance.org
SSRI antidepressants • SSRI = selective serotonin reuptake inhibitor • blocks reuptake of 5-HT, so concentration increases and more receptors are activated • SSRIs are the most common drug treatment for major depressive illnesses, and are also used to treat anxiety disorders
Effects of two SSRIs on Hamilton Depression Rating scores in a randomized, double-blind, placebo-controlled study of 316 patients with major depressive disorder (from Stahl 2000, Biological Psychiatry 48, 894-901) sertraline v placebo: p < .05 at weeks 12, 20 & 24 citalopram v placebo: p < .01 at weeks 4 to 24
Serotonin & mood • as with ATD, effects of SSRIs in non-depressed subjects are seen in changes in subjective feelings of hostility, aggression & irritability • increasing levels of 5-HT with SSRIs in non-depressed subjects reduces hostility & irritability • and increases ‘social affiliation’ and co-operative behaviours
Effects of 20mg/day SSRI (paroxetine) in normal volunteers – Knutson et al 1998, American Journal of Psychiatry 155, 373-379
Scores for co-operative behaviour in a 2 person (1 SSRI & 1 placebo) problem-solving task. Behaviour was filmed using hidden camera and scorers were blind to condition.
Serotonin & cognition • serotonin appears to play an important role in – • memory (hippocampus is rich in 5-HT receptors) • tasks that require response inhibition (e.g. Stroop tasks) • processing emotional information (e.g. facial expressions)
Serotonin & memory • ATD generally impairs memory performance • however - impairment may be for emotionally neutral and positive stimuli only, with memory for negative emotional stimuli unaffected or even improved (mood-congruent memory bias) • see Merens et al (2007)
Serotonin & the Stroop task • ATD may reduce interference in the Stroop task
Serotonin & the Stroop task • e.g. Evers et al (2006), NeuroImage 32, 248-255 • interference score = extra time needed for colour-incongruent words compared to colour-congruent words
Serotonin & facial expression processing • 5-HT manipulations affect recognition of emotions – • reducing levels of5-HT with ATD impairs recognition of fear & happiness in ‘normal’ subjects • increasing levels of 5-HT with SSRIs enhances recognition of fear & happiness • see Merens et al (2007)
Mechanism of action of SSRIs • some researchers have hypothesised that changes in cognition (memory biases, face processing, etc.) are basis for mood-enhancing effects of SSRI antidepressants • could explain delay between physiological & behavioural effects – it may require several weeks for cognitive changes to build up to a clinical (i.e. mood) effect • see Merens et al (2007)
‘Hallucinogens’/ ‘Psychedelics’ • LSD, psilocybin, mescaline - • share ‘indole ring’ structure with serotonin • ‘hallucinogen’ = ‘causing hallucinations’, but frank hallucinations are actually rare • ‘psychedelic’ = ‘mind revealing’
Lysergic acid diethylamide (LSD) “Objects appeared to gain in relief; they assumed unusual dimensions; and colours became more glowing. Even self-perception and the sense of time were changed. When the eyes were closed, there surged upon me an uninterrupted stream of fantastic images of extraordinary plasticity and vividness and accompanied by an intense, kaleidoscope-like play of colours.” (Albert Hofmann, discoverer of LSD, 1943)
‘Hallucinogens’ / ‘Psychedelics’ • structure suggests action at 5-HT receptors, but… • increasing serotonergic activity with buspirone or SSRIs doesn’t produce ‘hallucinogenic’ or ‘psychedelic’ effects, • and neither does reducing serotonin levels through acute tryptophan depletion
‘Hallucinogens’ / ‘Psychedelics’ • research shows that these drugs produce their effects mainly by acting as serotonin agonists • but only at some sub-types of 5-HT receptors (& may act as antagonists at others) • a sub-type of 5-HT receptor found in the prefrontal cortex (PFC) and thalamus is the main site of agonistic action
‘Hallucinogens’ / ‘Psychedelics’ • PFC – ‘high level’ cognitive processes and subjective experience of ‘self’ • thalamus – ‘sensory relay station’ receiving inputs from sense organs, and projecting to cortex • disruption of these systems could be basis for ‘psychedelic’ and hallucinatory experiences
MDMA – acute effects • MDMA is a modified amphetamine - it increases release of both DA & NA, so has psychostimulant properties • also increases release & inhibits reuptake of 5-HT, so has mood-enhancing & psychedelic properties • has additional subjective effects not seen in other drugs - increased emotional sensitivity & empathy • these led to MDMA and similar drugs (MDA, MDE) being classed as ‘entactogens’ (Nichols, 1986) or ‘empathogens’ (Metzner, 2001)
MDMA – sub-acute effects • users often report ‘midweek blues’ after taking MDMA at weekends • low mood, lethargy, irritability, difficulty concentrating • thought to be caused by depleted levels of monoamine NTs • symptoms are similar to effects of acute tryptophan depletion (ATD) in lab studies
MDMA – effects of chronic use • many (~80%) long-term, heavy users report an increased incidence of depression, anxiety & sleep disorders • cognitive impairments are seen in frontal-executive functions (planning, problem solving) & memory tasks in studies of heavy users • may be due to damage to 5-HT nerve axons in the cerebral cortex & hippocampus (see Parrott, 2002)
Free recall of word lists in MDMA users (Parrott & Lasky 1998, Psychopharmacology 139, 261-268) • light grey = non-user control group • dark grey = novice (<10 times) MDMA users • white = regular MDMA users
Serotonin (5-HT) - summary • 5-HT has a primarily inhibitory function & often acts in opposition to acetylcholine, noradrenaline & dopamine • important role in sleep, mood, pain & temperature regulation • also modulates cognitive function – especially memory, response inhibition & perception of emotional stimuli (e.g. faces) • 5-HT levels can be manipulated by dietary interventions – tryptophan supplements increase 5-HT, tryptophan depletion reduces 5-HT • acute tryptophan depletion (ATD) is associated with negative mood (irritability, aggression, depression) • increased serotonergic neurotransmission is associated with positive mood & pro-social behaviour,and is the basis for action of SSRI anti-depressants (e.g. Prozac) & subjective effects of psychedelic drugs (LSD, Ecstasy) • long-term, heavy use of Ecstasy is associated with increased incidence of mood & sleep disorders, and with impaired cognitive function (especially in frontal executive & memory tasks)
Learning outcomes • Understand how the manipulation of brain serotonin affects mood, cognition and social behaviour in humans. • Understand how SSRI antidepressants work, both in terms of their acute effects and how these may lead to a clinically significant improvement in mood. • Understand the acute, sub-acute and long-term effects of MDMA/Ecstasy use and their psychopharmacological basis.
Recommended reading • PJ Cowen (2008) Serotonin and depression. Trends in Pharmacological Sciences 29, 433-436 • W Merens et al (2007) The effects of serotonin manipulations on emotional information processing and mood. Journal of Affective Disorders 103, 43-62 (read the introduction & discussion) • AC Parrott (2000) Human research on MDMA neurotoxicity. Neuropsychobiology 42, 17-24 • AC Parrott (2002) Recreational Ecstasy/MDMA, the serotonin syndrome, and serotonergic neurotoxicity. Pharmacology, Biochemistry & Behavior 71, 837-844 • SN Young & M Leyton (2002) The role of serotonin in human mood and social interaction. Pharmacology, Biochemistry & Behavior 71, 857-865

![[lecture#5]](https://cdn0.slideserve.com/109460/slide1-dt.jpg)