Download
1 / 65
650 likes | 676 Views
Benign Prostatic Hyperplasia. İbrahim Umur Kepsutlu | Orhun Ufuk Tipi | Zeynepgül İnkaya. Προστάτης ( prostátēs ) : protector , guardian. Functions. P articipates in the control of urine output from the bladder and in the transmission of seminal fluid during ejaculation.

E N D
BenignProstaticHyperplasia İbrahim Umur Kepsutlu | Orhun Ufuk Tipi | Zeynepgülİnkaya
Προστάτης (prostátēs) : protector, guardian
Functions • Participates in the control of urine output from the bladder and in the transmission of seminal fluid during ejaculation. • Contributes to the seminal plasma a spectrum of small molecules and enzymes like fibrinolysin, coagulase which facilitate fertility. • Safeguards sperm viability by reducing the acidity of the urethra. • It facilitates and enhances sperm motility by contributing albumin to seminal plasma. • Prostatic acid phosphataseis involved in the nutrition of spermatozoa. • Secretes a high level of zinc to human seminal plasma which acts as an antibacterial agent.
Constituents • 30% of semen.
Location • posterior to the pubic symphysis • superior to the perineal membrane • inferiortothebladder • anteriortotherectum
Dimensions • 20 gr, • 3 cm in length, • 4 cm in width, • 2 cm in depth.
Histology • GlandularTissue & FibromuscularStroma
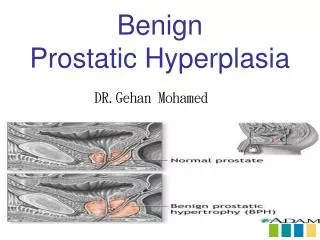
Definition • Genelde prostatın transitionalzonunda, sekretuar ve stromal hücrelerin çoğalması ile karakterize • Progressive • Nonmalign • Prostat büyümesine bağlı mesane çıkımında gelişen obstrüksiyon ve buna sekonder alt üriner sistem disfonksiyon belirtileri
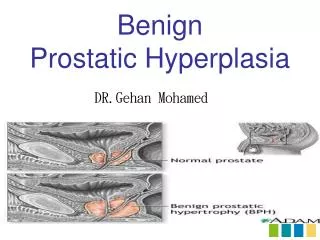
Etiology • Increasednumber of epithelialandstromalcells in periurethralarea of prostate (Hyperplasia)
Production/Destruction Epithelialorstromalproliferation Androgens Impairedprogrammedcelldeath
StemCells • Stemcells of prostate • Transientlyproliferativecells Block • Programmedcelldeath
Androgens • Withincreasingage: • Testosterone • Dihydrotestosterone • Androgenreceptors • Estradiol/Bioavailabletestosterone
But… • Theprostaticandrogen is: Dihydrotestosterone (90% Testicles, 10% Adrenals) 5αredüktaz Testosterone DHT
5αredüktaz • Type 1 >>>Skin andliver • Type 2 >>> Prostate *Can be inhibitedbyFinasterideandDutasteride *Theportionthat is in stromalcells is thekeyto androgenicamplification.
Estrogens • May play a role in induction of AndrogenReceptors (AR) • May increasetheamount of Ars • ER-α >>> Stromal ER-β >>> Epithelial • Intraprostaticestrogenisincreased in BPH ?
GrowthFactors • Keratinocytegrowthfactor (KGF) • Epidermalgrowthfactor (EGF) • Insulin-likegrowthfactor I-II (IGF 1-2) • Fibroblastgrowthfactor (FBF) • Transforminggrowthfactor (TGF)
GeneticsandFamilialFactors • Familial BPH Surgery in age<60 Prostatevolume = 82.7 mL 3 ormorerelatives in familyhistory • Sporadic BPH Surgery in age>60 Prostatevolume = 55.5 mL
Pathophisiology • Anatomicalobstruction • Primaryobstruction (Pressureincrease in proximal of obstruction) • Secondaryobstruction (Retention – Infection – Hydronephrosis)
Prostatehyperplasia Increasedurethralresistance Compensatorychanges in bladder ElevateddetrusorDecreasedstorage pressurefunction + Agerelatedchanges Urinaryfrequency, Urgency, Nocturia
Bladder’sresponse • Beginningphase • Compensatoryphase • Normal pressure • Morphologicalchanges in smoothmuscleandcollogen • Trabeculation, Diverticulation, Cellule • Decompensatoryphase • Muscletissue is replacedbyconnectivetissue • Increase in bladderweight • Increase in pressure • Detrusorinstability
ObstructionBladderchanges Detoriation of urinarystream, hesitancy, intermittency, increasedresidualurine Symptoms of frequencyandurgency Decreaseddetrusorcontractility Detrusorinstability + Decreasedcompliance
Inlaterstages… • Bilateralureterectasia • Uretohydronephrosis • Chronickidneyfailure
Epidemiology • Not seenbeforeage of 30. • 40 years 8% • 50 years 40% • 70 years 70% • 80 years 90%
Diagnosis • History • SymptomScore • PhysicalExamination (DRE) • VoidingDiary • Urinalysis, Culture • PSA • Uroflowmetry • PVR • Creatinine
Symptoms Obstructive • Slow stream • Incontinance • Terminal dribbling • Splitting/ Spraying • Hesitancy Irritative • Pollakiuria • Nocturia • Dysuria • Urgency
Semptomlar spesifik değil! • Prostat büyüklüğü ile semptom şiddeti kesin bağlantılı değil!
SymptomScoring • Madsen-IversenSymptomScoreforBenignProstaticHyperplasia • BoyarskySymptomScoreforBenignProstaticHyperplasia • AUA • InternationalProstateSymptomScore (IPSS) • Disease-SpecificQuality-of-Life ( QOL)
Question eight refers to the patient’s perceived quality of life. The first seven questions of the I-PSS are identical to the questions appearing on the AmericanUrological Association (AUA) Symptom Index which currently categorizes symptoms asfollows: • Mild (symptom score less than of equal to 7) • Moderate (symptom score range 8-19) • Severe (symptom score range 20-35)
DigitalRectalExamination • A digital rectal exam checks the size and firmness of theprostate. But the size of the prostate does not always determine the severity of the symptoms.
Urinalysis • A urinalysis and urine culture check for a urinarytractinfection that might be the cause of the symptoms. • Urinalysis—examination of a urine sample under a microscope—is performed in all patients who have lower urinary tract symptoms. Urinalysis is often the only laboratory test needed when symptoms are mild (International Prostate Symptom Score of 1 to 7) and the medical history and physical examination suggest no other abnormalities. • Urine culture (an attempt to grow and identify bacteria in a laboratory dish) is performed when a urinary tract infection is suspected.
PSA • Prostat spesifik antijen (PSA) prostat epitel hücrelerinden salgılanan glikoprotein yapıda bir proteazdır. • Helpscheck for prostate cancer, which can cause the same symptoms as BPH. • PSA values alone are not helpful in determining whether symptoms are due to BPH or prostate cancer because both conditions can cause elevated levels. However, knowing a man's PSA level may help predict how rapidly his prostate will increase in size over time and whether problems such as urinary retention are likely to occur. • 0 to 4 ng/mL is considerednormal.(Recentlybeenchallengedandlowerthresholdshavebeenrecommended(<2.5 ng/mL))
Uroflowmetry • In this noninvasive test, a man urinates into an electronic device that measures the speed of his urine flow. A slow flow rate suggests an obstruction of the urethra. If the flow rate is high, urethral obstruction is unlikely, and therapy for BPH will not be effective in most instances. • A normal urine flow rate is 15 mL per second or higher. • Maksimum akım hızı < 10 ml/sn obstrüksiyon varlığını gösterir.
PVR • The post-void residual (PVR)urine test measures the amount of urine left in the bladderafter urination. • The test is used to help evaluate: • Incontinence,urination problemsand enlarged prostate(benign prostatic hyperplasia, or BPH). • The amount of leftover (residual) urine can be measured by draining thebladderwith a thin flexible tube (catheter) or by using ultrasound. The catheter method has a slight risk of causing infection or injury to the tube leading from the bladder (urethra). But the catheter method is safe when done carefully. And it may be less expensive than ultrasound. • 100 cc den fazla olan rezidüel idrar, boşaltım bozukluğunu işaret eder.
Pressure-FlowUrodynamicStudies • These studies measure bladder pressure during urination by placing a recording device into the bladder and often into the rectum. The difference in pressure between the bladder and the rectum indicates the pressure generated when the bladder muscle contracts. • A high pressure accompanied by a low urine flow rate indicates urethral obstruction. A low pressure with a low urine flow rate signals an abnormality in the bladder itself, such as one related to a neurological disorder.
AdditionalMethods • Cystoscopy • Ultrasonography (abdominal, renal, transrectal) • CT • MRI • IVU/IVP
TRUS • A useful tool that can help supplement various diagnostic and treatment modalities for prostate cancer is transrectalultrasonography(TRUS). TRUS has become an extension of the urologist’s finger in the early detection of prostate cancer. The evolution of end-firing probes has further enhanced urologists’ ability to monitor the entire process of a prostate biopsy.TRUS is also widely used to deliver treatments such as brachytherapy and to monitor cryotherapy treatment for prostate cancer.
Earlier studies concentrated on the ultrasonographic appearances of prostate abnormalities such as benign prostatic hyperplasia (BPH), carcinoma of the prostate (CAP), prostatitis, prostatic abscess, and prostatic calculi. Since the introduction of the PSA screening test and early detection of prostate cancer, the role of TRUS has changed; it is mainly used to visualize the prostate and to aid in guided needle biopsy.