Download
1 / 59
790 likes | 1.66k Views
BENIGN PROSTATIC HYPERPLASIA. This disease is described by ancient physicians such as Avicenna, Paracelsus and others. Location and function of the prostate The prostate is a small gland present only in men which is about the size of a chestnut. Location and function of the prostate

E N D
This disease is described by ancient physicians such as Avicenna, Paracelsus and others
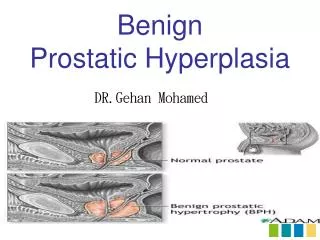
Location and function of the prostate • The prostate is a small gland present only in men which is about the size of a chestnut.
Location and function of the prostate • The prostate produces a fluid which forms a part of the semen. • During sexual intercourse, sperm pass from the seminal vesicles into the urethra and are carried through the urethra in fluid squeezed out from the prostate gland during orgasm.
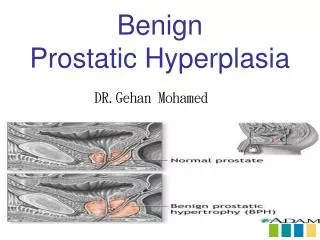
Enlargement of the BPH • In many, indeed, most men, the prostate progressively enlarges as they get older. • More than 50% of men over the age of 60 and 80% of men over the age of 80 have benign (i.e. not cancerous) enlarged prostates. • Doctors call this enlargement of the prostate 'benign prostatic hyperplasia' or 'BPH' for short.
Enlargement of the BPH • The prevalence of symptomatic BPH increases with age. • Beyond the age of 60 years, more than 40% of men are affected and almost half of these have significant impairment in quality of life.
Enlargement of the prostate gland • As the prostate enlarges, it presses on the urethra, which is the tube that carries the urine and semen out of the body. • This causes obstruction, making it difficult to pass urine. It may also make you want to go to the toilet more often and empty the bladder incompletely.
BPH complications • UTI (5-10%) • Acute urine retention (0.4-6%) • Hematuria (2-3%) • Chronic kidney insuffiency • Bladder stones • Upper urinary tract dilatation
Bladder problems • Distension of the ureters and back pressure on the kidneys may produce tiredness and loss of appetite. • Because of the high pressures in the bladder, 'pouches' called diverticula may form at weak points in the bladder wall. This may result in the need to pass urine twice in rapid succession.
BPH stages • I. Compensation • II. Subcompensation • III. Decompensation
Quantification of symptoms • Symptoms should be quantified by using the International Prostate Symptom Score (I-PSS) and Quality of Life Assessment. • The scores derived allow this tentative classification of symptoms as shown in Table .
Physical examination Physical examination should assess: - Suprapubic area to rule out significant bladder tone - Sphincter tone Bulbocavernosus reflex plus brief assessment of motor and sensory function in lower body Digital rectal examination (DRE) This procedure should be performed to evaluate the prostate gland with regard to approximate size, consistency, shape, and abnormalities suggestive of prostate cancer.
Interpreting results of DRE • BPH and prostate cancer are two distinct diseases, although they may coexist in the same patient. Patients should be advised that no clear evidence exists that BPH predisposes to development of cancer.
Urinalysis It is used to determine if the patient has - Haematuria - Proteinuria • Pyuria Renal-function assessment - Should be determined by serum creatinine test
Uroflowmetry • Uroflowmetry, an non-invasive technique, is recommended in the initial diagnostic assessment and whenever appropriate during and after treatment to determine response . • Maximal urinary flow rate (Qmax) is the best single measure, but a low Qmax does not distinguish between obstruction and decreased bladder contractility.
Ultrasonography Residual urine • The determination of residual urine is recommended in the initial diagnostic assessment of the patient during and after treatment to determine response.
Prostate specific antigen • PSA is an important indicator of prostate cancer because it is a protein secreted exclusively by prostatic epithelial cells and is elevated in the serum of most patients with BPH or prostate cancer.
X-Ray Examination • Excretory urography • Retrograde cystography • Retrograde urethrography gives only indirect information on the effect of benign prostatic enlargement (BPE) on adjacent structures.
Cystoscopy • The standard endoscopic procedure for diagnostic evaluation of the lower urinary tract (urethra, prostate, bladder neck and bladder) is a urethrocystoscopy. • This investigation can confirm causes of outflow obstruction while eliminating intravesical abnormalities.
Treatment of BPH • Most treatments for prostate enlargement aim to reduce the size of the prostate and its restrictive effect on the urethra. • This may be done either with drugs or by surgery. • Those with only minor symptoms need no treatment. This is sometimes called 'watchful waiting'.
Treatment of BPH
Treatment of prostate enlargement • In general, if symptoms are mild or moderate, either no treatment or treatment with tablets will be tried at first. • The risk of side-effects with tablets is small and they usually disappear if treatment is stopped.
Contraindications to medical treatment of BPH • Acute urinary retention • Palpable bladder, large volume of post-void residual urine (>300ml) • Renal insufficiency • Recurrent haematuria • Recurrent urinary tract infections secondary to BPH • Bladder stones or diverticula • Evidence of prostate cancer
Non-invasive methods • Transurethral Laser Interstitial Ablation • Transurethral Laser Needle Ablation • Transurethral Microwave thermotherapy • High Intensity Focused Ultrasound • Intraprostatic stents
Operative treatment • Indications:Medication is ineffective • Residual urine • Repetitive urine retention • Upper urinary way dilatation • Hematuria • Recurrent UTI • TURP – transurethral prostatectomy(“gold standart”) • TUIP –Transurethral incision of prostate • Open operation
Transurethral incision of the prostate (TUIP) • Transurethral incision of the prostate (TUIP) is not the most common prostate operation, but may be the most suitable procedure when the prostate is still quite small, and is becoming increasingly popular with urologists.
Transurethral resection of the prostate (TURP) • TURP is the most frequently performed operation for BPH. • It is carried out under a general anaesthetic and usually takes about 30-60 minutes. TURP involves passing an instrument up the urethra and cutting away the middle of the enlarged prostate.
Retropubic prostatectomy (RP) • Retropubic prostatectomy (RP) is an operation that is usually performed only if the prostate is very large by means of a cut through the skin.
Prostatic stents Stents are small metal coils that are inserted into the urethra to hold the walls open. • Two types of stent are available - temporary and permanent.
Transrectal hyperthermia • Transrectal hyperthermia uses microwave energy to destroy some of the prostate tissue by heat. • The procedure is carried out without anaesthesia and takes about 60 minutes;
Transurethral thermotherapy • Transurethral thermotherapy uses microwave energy to destroy some of the prostate tissue by heat. • The procedure is carried out under local anaesthesia, which means that you will be awake throughout the operation, which takes about 60 minutes.
Laser therapy • Laser energy is used to destroy some of the prostate tissue by intense local heat. The procedure is carried out under a general anaesthetic and takes about 20 minutes.
High intensity focused ultrasound therapy • High intensity focused ultrasound is a very new technique that is used to destroy some of the prostate tissue by heat.
Prostate Cancer is n 'fifth place in the disease in men after 45 years
prostate cancer • In 1995, were approximately 244 000 new cases and 44 000 deaths from prostate cancer (PC)-numbers that will continue to rise as the population ages . Ninety-five percent of prostate cancer is diagnosed in men between 45 and 89 years of age with a median age of diagnosis of 72 years.
T Primary tumour Tx Primary tumour can not be assessed T0 No evidence of primary tumour T1 Clinically inapparent tumour not palpable or visible by imaging T1a Tumour incidental histological in 5% or less of tissue resected T1b Tumour incidental histological finding in more than 5% of tissue resected T1c Tumour identified by needle biopsy because of prostate specific antigen T2 Tumour confined within the prostate T2a Tumours involves one lobe T2b Tumour involves both lobes T3Tumours extends through the prostatic capsule T3a Extracapsular extension (uni- or bilateral) T3b Tumour invade Seminal vescile(s) T4 Tumour is fixed or invades adjacent structures other than seminal vesicles: bladder neck, external sphincter, rectum, levator ani and/or pelvic wall Classification of CaP