Download
1 / 18
190 likes | 541 Views
Peter Ofware, Peter Ouma, Amek Nyanguara, Adazu Kubaje, Milton Njeru, T. Akun, Vandenhoudt Hilde, Mary Hamel and Kayla Laserson KEMRI/CDC Field Research Station. The Magnitude and Causes of Maternal Mortality in Rural Western Kenya, 2003-2005. Background (1).

E N D
Peter Ofware, Peter Ouma, Amek Nyanguara, Adazu Kubaje, Milton Njeru, T. Akun, Vandenhoudt Hilde, Mary Hamel and Kayla Laserson KEMRI/CDC Field Research Station The Magnitude and Causes of Maternal Mortality in Rural Western Kenya, 2003-2005
Background (1) • Maternal mortality remains disturbingly high in developing countries • Each year ≈ 529,000 women, mainly from developing countries, are estimated to die from complications of pregnancy (UNFPA, 2004)
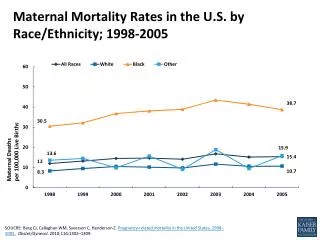
Background (2) • The recent inclusion of maternal health as one of the key UN Millennium Development Goals (MDGs) has increased its visibility on the world agenda • Estimates for Kenya: • 414 maternal deaths/100,000 live births (KDHS, 2003)
v Yala Sub D.H. v Siaya D. H. Gem Kisian Karemo * * v Asembo v Kombewa Sub D.H. Bondo D. H. Kisumu v Lwak H. 0 1 0 2 0 K i l o m e t e r s Continuous demographic monitoring of a geographically defined population of 220,000 individuals in Bondo and Siaya districts, Nyanza province Demographic Surveillance System (DSS)
Study Rationale • No definitive studies have been done to quantify the actual burden of maternal mortality in the DSS • Poor health indicators in the study area, thus MMR figures expected to be higher than national average • In the DSS, ante-natal care (ANC) is high (90%) but the majority (80%) deliver at home • Data would facilitate the design of appropriate interventions and contribute to national policy development
Study Objectives • To estimate the magnitude of maternal mortality in the DSS during the years 2003-2005 • To describe the causes of maternal mortality in the DSS during the years 2003-2005
Methods 1 (Definitions) • Maternal mortality • The death of a woman while pregnant, or within 42 days of termination of pregnancy from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes (WHO, 2004). • Maternal mortality ratio (MMR) • Number of maternal deaths during a given time period per 100,000 live births during the same period.
Methods 2 (Definitions) • Direct causes of maternal mortality • Causes resulting from pregnancy and delivery complications • Indirect causes of maternal mortality • Maternal deaths not related to pregnancy and delivery
Methods (3) • Data on births, deaths, in and out-migration collected 3 times a year • Causes of death determined by verbal autopsy • Analysis was done using SAS software version 9 (SAS, INC, North Carolina, USA • Maternal mortality calculated as the ratio of maternal deaths to live-births
Year MMR per 100,000 LB 2003 622 2004 647 2005 387 Overall 553 Magnitude of Maternal Mortality in the DSS
Causes of Maternal Mortality During Pregnancy/Delivery, 2003-2005
Causes of Maternal Mortality 42 Days After Delivery, 2003-2005
Limitations • Possible under-reporting of pregnancies • Possible under-reporting of maternal deaths and/or live births • Accuracy of verbal autopsy reports (respondent recall bias etc.) • Accuracy of expert panel review of VA (misclassification) • Significant reduction in MMR between 2004 and 2005 not fully explained
Conclusions • Overall 43% of the total maternal deaths occurred as a result of direct causes • Direct: Puerperal sepsis and abortion-miscarriage were the leading causes of death (28% and 17%) • Indirect: HIV/AIDS was the leading single cause of maternal mortality in the area (40%) • Maternal mortality in the study area is significantly higher than national average (553 vs. 414, P< 0.05) but decreasing
Recommendations • To reduce the direct causes, emphasis on safe abortion/miscarriage and “clean deliveries" could reduce MMR • Scaling up of HIV prevention and care could also reduce maternal mortality
Acknowledgments • Communities in Asembo and Gem • All the DSS Community interviewers • All the DSS Data management team • KEMRI/CDC Scientific team • VA expert panel group