Download
1 / 38
400 likes | 932 Views
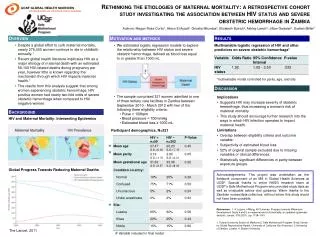
Maternal Mortality. Liliana Carvajal Vibeke Oestreich Nielsen Armando H. Seuc UNICEF Statistics Norway WHO. Background. MDG 5: Improve Maternal Health. Target 5.A: Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio 5.1 Maternal mortality ratio (MMR)

E N D
Maternal Mortality Liliana Carvajal Vibeke Oestreich Nielsen Armando H. Seuc UNICEF Statistics Norway WHO 08_XXX_MM1
Background 08_XXX_MM2
MDG 5: Improve Maternal Health • Target 5.A: Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio • 5.1 Maternal mortality ratio (MMR) • 5.2 Proportion of births attended by skilled health personnel (SAB) • Target 5.B: Achieve, by 2015, universal access to reproductive health • 5.3 Contraceptive prevalence rate • 5.4 Adolescent birth rate • 5.5 Antenatal care coverage • at least one visit and at least four visits • 5.6 Unmet need for family planning 08_XXX_MM3
Maternal Mortality • Target 5.A: Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio • 5.1 Maternal mortality ratio • 5.2 Proportion of births attended by skilled health personnel • Initially updates every 5 year since 1990 by WHO, UNICEF, UNFPA – The World Bank joined in 2005 • 2008 update – An academic team at University of Berkeley in collaboration with MMEIG • 2010 update – idem 08_XXX_MM4
Measuring Maternal Mortality 08_XXX_MM5
Trends in Maternal Mortality: 1990 to 2008 • Reviewed by the technical advisory group (TAG) with experts from academic institutions: Berkeley, Harvard, Hopkins, Texas, Aberdeen, Umea, Statistics Norway • Countries consulted for comments on methodology and additional input 08_XXX_MM6
Trends in Maternal Mortality: 1990 to 2010 • Reviewed by the technical advisory group (TAG) with experts from academic institutions: Berkeley, Harvard, Hopkins, Texas, Aberdeen, Umea, Statistics Norway • Countries consulted for comments on methodology and additional input 08_XXX_MM7
General framework of the maternal mortality estimates 1990-2008 and 1990-2010 • Levels and trends of maternal mortality between 1990 and 2008 for 172 countries (1990-2010 for 181 countries) • Hierarchical/multilevel linear regression model • The model input data is the PMDF (proportion maternal among all female deaths 15-49) adjusted for completeness and definition • Covariates: the log(GDP), log(GFR) and SAB • The final output takes into account the maternal mortality related with the HIV/AIDS 08_XXX_MM8
Definitions used • Maternal death: “the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes.” ICD-10, WHO,1994 • Pregnancy-related death: “the death of a woman while pregnant or within 42 days of termination of pregnancy” 08_XXX_MM9
Estimated measures • Maternal Mortality Ratio (MMR): Ratio of maternal deaths in a period to live births (proxy for risky events) in the same period (x 100,000). • Number of maternal deaths • PMDF: Proportion of maternal among female deaths 15-49 • Lifetime risk of a maternal death: An estimate of the likelihood that a woman who survives to age 15 will die of maternal causes • proportion of women reaching reproductive age who would die of maternal causes, taking into account competing causes 08_XXX_MM10
Input data to the model: PMDF • PMDF is considered less subject to under-reporting than MMR (maternal and non-maternal deaths likely to be under-reported to similar degree) • Maternal deaths as defined by ICD is difficult to capture – usually all deaths in pregnancy measured • Efforts have been made to adjust for: • under reporting • definition • For the model the HIV/AIDS component was taken out from the PMDF; the HIV/AIDS component is then added back after the model fitting 08_XXX_MM11
Input database • 1990-2008: Database of 172 countries - territories, from 1985 onwards • 1990-2010: Database of 181 countries - territories, from 1985 onwards • Nationally representative data => focusing on sources where PMDF is possible to compute 08_XXX_MM12
Methods of Data Collection, Estimation 08_XXX_MM13
Sources of Data • Civil registration systems with cause of death assigned by attending physician • Household surveys with sibling histories • Sample vital registration systems • Reproductive Age Mortality Surveys (RAMOS): not very common • Population censuses with questions on household deaths • Hospital- or facility-based studies • Other 08_XXX_MM14
Data on maternal mortality: availability 08_XXX_MM15 *: 1990-2010 estimations
Data available in the Region: • Civil registration characterized as complete, with good attribution of cause of death • Countries lacking good complete registration data but where other types of data are available • No national data on maternal mortality 08_XXX_MM16
General Problems with Maternal Mortality Measurement • Rare events • National trends unstable • For household surveys requires very large samples • Certain types of maternal deaths hard to identify (especially abortion-related) • Non-VR methods tend to measure pregnancy-related mortality PRMR 08_XXX_MM17
Civil Registration Data • WHO estimates that approx. 72 (out of 193) member states have complete recording of deaths • But not all have adequate cause of death data • Even in countries with complete VR, classification of deaths as maternal is problematic • Recent increase in MMR (47% 2002 to 2004) in US due to change of death certificate • Issues: • 14 studies (confidential enquiries, record linkages) of countries with complete registration: a median underestimation of 0.5 true maternal deaths were incorrectly recorded as non-maternal 08_XXX_MM18
Household Surveys With Sibling Histories • Key questions for sibling history: • Each sibling listed individually • Record sex • Record age in completed years for surviving sibs • Record year of death, age at death for dead sibs • For deaths of women of reproductive age, 3 questions about timing of death relative to pregnancy • Widely used by DHS program (41countries,65 surveys) • Issues: • Measures pregnancy-related mortality • Estimates are usually made for 7 years before survey • May under-estimate overall mortality 08_XXX_MM19
Sample Vital Registration Systems • Special procedures in random sample of areas (4,000+ in India, 160 in China) • Continuous monitoring of vital events plus 6-monthly household survey (India) • Cause of death identified by verbal autopsy (VA) (India) or case records plus VA (China) • Issues: • Requires considerable administrative sophistication • Cannot be implemented rapidly • Needs periodic evaluation 08_XXX_MM20
RAMOS Studies • Starting point is complete listing of deaths of women of reproductive age • Best starting point is close to complete VR • Key feature is triangulation among data sources (eg church records, burial grounds) to identify missed deaths • May be done for a sample (but has to be large) • Each death is investigated in detail to determine whether or not it was maternal • Hospital, health facility records • Household interviews • Issues: • Results may be no better than the frame of deaths • MMR also needs number of births 08_XXX_MM21
Censuses with Questions on Deaths • Population censuses can include questions on deaths in households in defined recent reference period • Reported deaths of reproductive aged women trigger questions about the timing of death relative to pregnancy • Issues: • Pregnancy-related mortality • Census misses deaths in single-person households • Death of head of household may result in household breakup • Experience suggests there is almost always some under-reporting • Need to evaluate carefully • No consensus as to the quality of the data obtained 08_XXX_MM22
Facility-Based Studies • Useful for identifying areas for improved care (confidential enquiries) • Potential for gold standard case identification (case notes) • Facility deaths (and births) are selected on characteristics that may not be known • Not readily generalizable to a national MMR estimate 08_XXX_MM23
Estimation (Modelling) 08_XXX_MM24
Modelling • Countries in Group A • No modelling was used • Essentially data from CR were adjusted by a 1.5 factor • Countries in Groups B and C • Multilevel model was used to predict PMDF with GDP, GFR and SAB as predictors • Group C countries «borrowed» from other countries in the region • PMDF was converted into MMR 08_XXX_MM25
Input data to the model:Adjustment by type of source • Adjustment for completeness of reporting specified in relation to the type of data • CR system: Review of recent literature on underestimation of maternal deaths in CR systems • adjustment by a factor of 1.5 • Sibling histories: age-standardization, • 1.1 adjustment (underestimation of early pregnancy deaths) • 0.9, 0.85 adjustment (remove accidental deaths) • Other special studies (e.g., RAMOS): • 1.1 adjustment 08_XXX_MM26
Covariates • GDP: gross domestic product PPP per capita, in constant 2005 international dollar; the World Bank series, complemented by other sources • GFR: general fertility rate, the number of births in a population divided by the number of women at reproductive ages; UNPD World Population Prospects • SAB: the proportion of deliveries with a skilled attendant at birth from UNICEF database 08_XXX_MM27
Covariates and the model • A time series of these three covariates were constructed for the 1985-2008 (1985-2010) period • Time-matched average values of the covariates for time intervals corresponding to the period of each observation of the dependent variable PMDF were computed • A hierarchical/multilevel model with three main covariates, plus random effects for countries and regions and an offset which will adjust the denominator of PMDF for AIDS. 08_XXX_MM28
Input data to the model:Definition and HIV/AIDS adjustment 08_XXX_MM29
Excluding AIDS-related deaths from PMDF: • PMDFadj1=(PMDFadj0 – ũ v a) (1-π)δ • removes from numerator • a = fraction of AIDS deaths among deaths to women aged 15-49 • v = proportion of such AIDS deaths that occur during pregnancy (or within 42 days after delivery) • ũ= fraction “actually" counted as maternal • log(PMDFadj1) = b0 + j + k + b1 log(GDP) + b2 log(GFR) + b3 SAB + log(1‐a) + ε • removes from denominator • AMDF = AIDS-adjusted (denominator) PMDF = (PMDFadj1)/(1-a)
Final estimates of PMDF: • PMDFa : splitting the UNAIDS estimate of total AIDS deaths among women aged 15‐49; PMDFa = u v a a = fraction of AIDS deaths among deaths to women aged 15-49 v = proportion of such AIDS deaths that occur during pregnancy (or within 42 days after delivery) u = fraction that “should be" counted as maternal • PMDF = PMDFna + PMDFa
Uncertainty Components of uncertainty include: • Any remaining bias in adjusted PMDF values • Uncertainty in model parameters (c, k, u, and pi) • Regression prediction uncertainty within the PMDF model • Possible error in MMR conversion (estimated births and deaths) • Alternative models, covariates, etc. 08_XXX_MM34
What is new in 2008 and 2010 compared with 2005 • Trend estimates for countries => bigger database • Definition issue addressed • Maternal deaths related with HIV/AIDS taken into account • Statistical model – more detailed 08_XXX_MM35
Whatis new in 2010 comparedwith 2008 • Data availability: • 3200 country-years of data in 2010 comparedwith 2842 in 2008 (13% increase) • Total femaledeaths in the reproductive agewereupdatedbackward (routine updatingprocess by WHO) • Countries included: • 181 in 2010 vs. 172 in 2008. The population cut-off for country inclusion was 100000 in 2010 vs. 250000 in 2008 08_XXX_MM36
Country consultation 08_XXX_MM37
Country consultation • CL.33.2011 (8 December 2011): • “Following WHO’s quality standards for data publication and prior to the official release of the above estimates, WHO is consulting with its Member States to review each individual country estimate in order to identify and make use of primary data sources that may not have been previously identified.” • Focal point identification and review. Comments received during consultation. • Accepted amendments to data input • source of reference clearly identified 08_XXX_MM38