Download
1 / 18
190 likes | 621 Views
STREPTOCOCCUS INTERMEDIUS VERTEBRAL OSTEOMYELITIS AND ENDOCARDITIS . Capt. Mauricio De Castro (ACP associate), USAF, MC Maj. Robert Holmes (ACP member), USAF, MC Keesler Medical Center. CASE PRESENTATION.

E N D
STREPTOCOCCUS INTERMEDIUS VERTEBRAL OSTEOMYELITIS AND ENDOCARDITIS Capt. Mauricio De Castro (ACP associate), USAF, MC Maj. Robert Holmes (ACP member), USAF, MC Keesler Medical Center
CASE PRESENTATION • 49-year-old male with history of chronic back pain being followed by the Neurology service • Patient treated unsuccessfully with analgesics and muscle relaxants • Presented with acute exacerbation of back pain following heavy lifting, MRI was ordered
MEDICAL PROBLEM LIST • Torticollis • GERD • Hypertension • Bilateral shoulder surgeries 03’ and 04’ • Bilateral inguinal hernia repairs • Acne
Baclofen Diazepam Zolpidem Acetaminophen/Oxycodone Lidocainetransdermal patches Esomeprazole CURRENT MEDICATIONS
SOCIAL HISTORY • Remote tobacco use • Infrequent ethanol consumption • No illegal substance or prescription drug abuse • No transfusions • No pets or recent travel
Admitted that day for fluoroscopy guided inter vertebral disc space biopsy and PICC placement Serial blood cultures were drawn over several days Initial biopsy grew Streptococcus intermedius, because of potentially contaminated study another biopsy was done CASE PRESENTATION
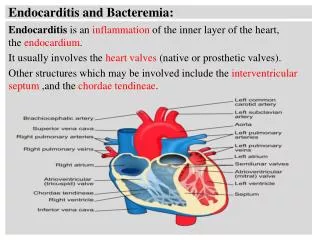
CASE PRESENTATION • After one blood culture bottle turned positive a transesophagic echocardiogram was performed • TEE showed 1cm vegetation on anterior leaflet of mitral valve consistent with infective endocarditis (IE) • No additional microbiological samples were ever positive
CASE PRESENTATION • On admission and throughout hospitalization all of the patient’s labs were normal to include: • CBC • Comprehensive metabolic panels • Inflammatory markers • An extensive evaluation of the following failed to identify a source: • Skin exam • Dental exam to include a panoramic X-ray • Esophagastroduodenoscopy • Digital rectal exam • Urinalysis • Urine culture
CASE PRESENTATION • The patient completed an initial two week course of intravenous gentamicin plus penicillin and a 16 week course of ceftriaxone after initial treatment • Subsequent TEE and serial MRI revealed resolution of the lesions
Streptococcus intermedius • Part of the ‘millerigroup’ (S. anginosus, S. constellatus), commensals of the mouth and upper respiratory tract • Infrequent pathogens in the Streptococcusviridans group • Propensity to colonize mouth and invade other organs
Streptococcus intermedius • Very rare cause of pyogenic infections, reported cases include: • Endocarditis • Osteomyelitis • Muscle abscess • Pneumonia • Abdominal abscess • Typically produce tiny caramel-smelling cultures on agar plates
COMBINED IE AND OSTEOMYELITIS • Osteomyelitis can complicate from 2-6% of all IE, while some series have reported up to 10% of vertebral osteomyelitis have concurrent IE • Dissemination route is usually hematogenous, thought to be through Batson’s plexus veins • A constant source of bacteremia is an excellent cause of either, determining the sequence of events can prove to be difficult
COMBINED IE AND OSTEOMYELITIS • Staphylococcusaureus and epidermidis account for up to 90% of isolated osteomyelitis and 30% of endocarditis • Organisms from Streptococcus viridans group are an infrequent cause of endocarditis and even more rare cause of osteomyelitis
COMBINED IE AND OSTEOMYELITIS • Osteomyelitis cause by organisms belonging to Streptococcusviridans group usually presents with severe lower back pain, fever and leukocytosis • Usual sources for these organisms include the GU tract, soft tissue infection and upper respiratory tract • Antibiotic regimes vary from 4 weeks to 6 months, depending on the author, 4-6 weeks of parenteral antibiotics is common practice
CONCLUSIONS • Although infrequent it’s important to recognize microorganisms from the ‘milleri group’ as potential pathogens in cases of vertebral osteomyelitis • Recognize that it might be hard to isolate this particular bacteria • May present as indolent disease with minimal inflammatory response
REFERENCES • Speechly ME, Swanton D, Swanton RH. Osteomyelitis and infective endocarditis. Postgrad Med J 1994;70:885-890 • Buchman AL. Streptococcus viridans osteomyelitis with endocarditis presenting as acute onset lower back pain. J Emerg Med 1990;8:291-295 • Barham NJ, Flint EJ, Mifsud RP. Osteomyelitis complicating streptococcus milleri endocarditis. Postgrad Med J 1990;66:314-315 • Spadafora PF, Qadir MT, Cunha BA. Streptococcus bovis endocarditis and vertebral osteomyelitis. Heart Lung 1996;25:165-168 • Roberts-Thomson PJ, Rischmueller M, Kwiatek RA, Soden M, Ahern MJ, Hill WR, Geddes RA. Rheumatic manifestations of infective endocarditis. RheumatolInt 1992;12:61-63 • Demers C, Tremblay M, Lacourciere Y. Acute vertebral osteomyelitis complicating streptococcus sanguis endocarditis. Ann Rheum Dis 1988;47:333-336 • Sapico FL, Liquete JA, Sarma RJ. Bone and joint infections in patients with infective endocarditis: review of a 4 year experience. Clin Infect Dis 1996;22:783-787