Download
1 / 41
470 likes | 835 Views
Polycythemia Vera. Andrea Brassard NURS 7724 November 25, 2002. Objectives. Upon completion of this program the participant will: 1. Define polycythemia vera (PV). 2. Describe the epidemiology of PV. 3. Identify the symptoms and signs of PV 4. Describe how PV is diagnosed.

E N D
Polycythemia Vera Andrea Brassard NURS 7724 November 25, 2002
Objectives Upon completion of this program the participant will: 1. Define polycythemia vera (PV). 2. Describe the epidemiology of PV. 3. Identify the symptoms and signs of PV 4. Describe how PV is diagnosed. 5. Identify therapeutic modalities for PV. 6. Identify the complications of PV.
PV: Definition • A chronic, progressive blood disorder • Caused by an abnormality in certain immature cells in the bone marrow • Stimulates an overproduction of RBCs, WBCs, & platelets http://hopkinsafter50.com/html/newsletter/ha0502
PV: Definition • A neoplastic (clonal) stem cell disorder • probably arising in a pluripotent hematopoietic progenator cell • which leads to excessive production of all myeloid cell lines • predominantly red blood cells (Wasserman, Berk, & Berlin, 1995)
Epidemiology of PV • Relatively rare disorder • Annual incidence 0.6 to 1.6 per million per year • Ages 50 to 70 peak years • Slightly more prevalent in males • More common in Jews, less common in blacks • Possible genetic predisposition
PV: Symptoms • The symptoms and signs of PV can be attributed to the expanded total blood volume and the increased blood viscosity. • The onset of PV is insidious and symptoms frequently precede a diagnosis of PV by several years. • Patients may be asymptomatic or have vague or non-specific complaints
Symptoms of PV A large study of PV revealed the following symptoms and reported frequency headache (48%) weakness (47%) pruritus(43%) dizziness (43%) sweating (33%) visual disturbances (31%) weight loss (29%) paresthesias (29%) dyspnea (26%) joint symptoms (26%) epigastric distress (24%) (Wasserman, Berk, & Berlin, 1995)
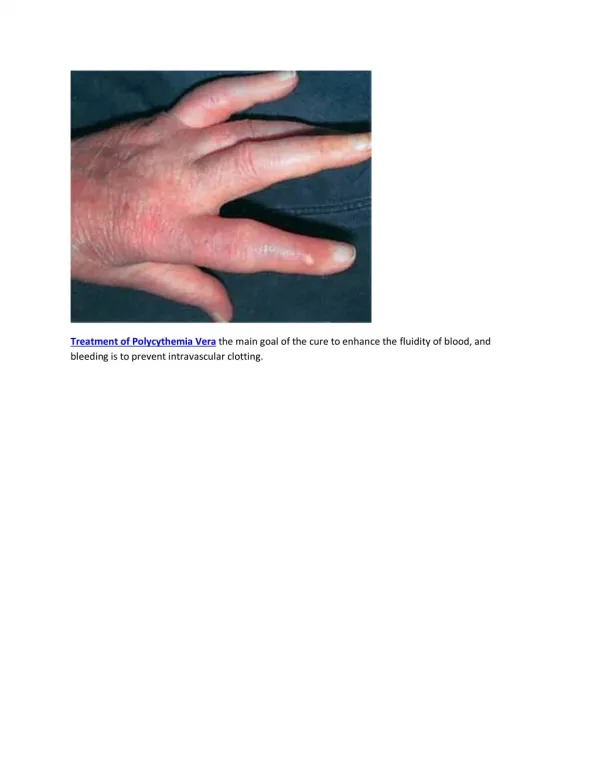
Signs of PV on Physical Exam • Enlarged spleen (70%) • Skin plethora (ruddy cyanosis) (67%) • Conjunctival plethora (59%) • Fundoscopic - engorged vessels (46%) • Enlarged liver (40%) • Systolic B/P > 140 (72%) • Diastolic B/P > 90 (32%) (Wasserman, Berk, & Berlin, 1995)
Diagnosis of PV • Elevated hematocrit is first clue • REFER TO HEMATOLOGIST! • Additional Diagnostic tests include: CBC and peripheral smear Bone marrow aspiration and biopsy Leukocyted alkaline phosphatase Abdominal ultrasound and/or CT; IVP Erythropoetin level; Serum B12; ABG
Laboratory features in PV • Elevated red cell mass • Red cell morphology • Leukocytosis • Mild basophilia • Mild to moderate thrombocytosis
PV: Typical CBC WBC 18 [4-11] Neuts 14 [2-7.5] hgb 20 [14-18] Lymphs 2 [1.5-4] hct 62 [42-51] Monos 0.8 [.2-.8] MCV 75 [80-100] Eos 0.1 [0-0.7] Platelets 850 [150-450] Basos 0.5 [0-0.1]
Bone marrow features in PV Hypercellularity and hyperplasia of • erythroid • granolocytic • megakaryocytic cell lines
Major criteria 1. Total red cell mass Male >36 Female >32 2. Arterial oxygen saturation > 92 3. Splenomegaly Minor criteria 1. Thrombocytosis (platelets > 400) 2. Leukocytosis (WBC > 12) 3. Increased leukocyte alkaline phosphates (LAP) score 4. Serum B12 >900 PVSG Criteria for the diagnosis of Polycythemia Vera
Criteria for diagnosis of PV According to the Polycythemia Vera Study Group: • All 3 major criteria OR • The first 2 major criteria (increased red cell mass and O2 >92%) and two minor criteria.
Treatment of PV • Treatment approaches based on degree of thrombosis risk. • Risk factors include age, platelet count (>1,500 high risk), and pregnancy. • Low risk - phlebotomy alone or with low-dose aspirin. • Intermediate risk - add interferon alpha • High risk - add hydoxyurea
PV Therapeutic Modalities • Phlebotomy • Cytostatic agents • Radioactive Phosphorus • Hydroxyurea • Interferon-alpha • Anagrelide • Stem Cell Transplant
Phlebotomy • First choice for erythrocytosis • Target hct <45 • Remove 250 to 500 cc of blood q.o.d. • In elderly remove 200 to 300 cc b.i.w.
Phlebotomy Unfortunately, none of this blood is donated. Phlebotomized blood is discarded!
Phlebotomy alone will NOT control • thrombocytosis • leukocytosis • painfully enlarging spleen • hyperuricemia or • pruritis Patients treated with phlebotomy alone have high incidence of fatal or disabling thrombotic events. (Wasserman, Berk, & Berlin, 1995)
Cytostatic Agents for Myelosuppression • Leukeran was commonly used. • But leukeran increased leukemia risk • Other drugs: • melphalan • cyclophosphamide • busulfan • but risk of life-threatening thrombyocytopenia
Radioactive Phosphorus • Has been used for more than 50 years • Administered IV • No radiation sickness • Ameliorates abnormal physical findings • bright red skin color disappears in most • about 2/3 of enlarged spleens and livers become non-palpable after treatment (Wasserman, Berk, & Berlin, 1995)
Hydroxyurea • Used in patients in whom phlebotomy is problematic • Brand name “Droxia” • Administered p.o. • Warning! - drug is mutagenic • Side effects include rash, GI complaints, oral ulcers, fever.
Recombinant Interferon-alpha • PV is an off-label indication • t.i.w. subcutaneous injection • can reduce frequency of phlebotomy • spleen size reduced • Cost $50 to 150 per injection • Side effects - depression and suicidal ideation, flu-like symtpomes
Anagrelide • Platelet inhibitor • FDA approved 1997 “Orphan Drug” • Cost $600/month • Usual dose: 0.5 to 1 mg b.i.d. p.o. • Adverse effects - positive inotropic effect • Use caution in heart disease, renal insufficiency, hepatic dysfunction
Stem Cell Transplant • Recent study at Fred Hutchinson Cancer Research Center, Seattle, WA • 25 patients with advanced essential thrombocythemia (n=13) or PV (n=12) received stem cell transplants. • 64% three year survival rate
PV Complications and Treatment • Hyperuricemia - treat with allopurinol • Peptic ulcer disease - conventional Rx • Acute leukemia- poor prognosis • Thromboembolic risk - aspirin use controversial • Hemorrhagic complications - blood and/or platelet transfusions
References Hobbbrand, A.V., & Pettit, J.E., 1988. Sandoz Atlas of Clinical Hematology. London: Gower Medical. Lee, 1999. Wintrobe’s Clinical Hematology, 10th Ed. Philadelphia: Lippincott, Williams, & Wilkins. Mazza, J.J., 2002. Manual of clinical hematology, 3rd Ed. Philadelphia: Lippincott, Williams, & Wilkins. Mosby’s Drug Consult, 2002. Tefferi, A, Solberg, L.A., & Silverstein, M.N., 2000. A clinical update in polycythemia vera and essential thrombocythemia. American Journal of Medicine, 109, (2), 141-149. Wasserman, L.R., Berk, P.D, & Berlin, N.I., 1995. Polycythemia Vera and the myeloproliferative disorders. Philadelphia: Saunders.