Download
1 / 1
10 likes | 232 Views
Initial experience with sequential BCG / Electro-motive drug administration (EMDA) Mitomycin-C (MMC) as the standard intravesical regimen for high risk non-muscle invasive bladder cancer (NMIBC). p50.

E N D
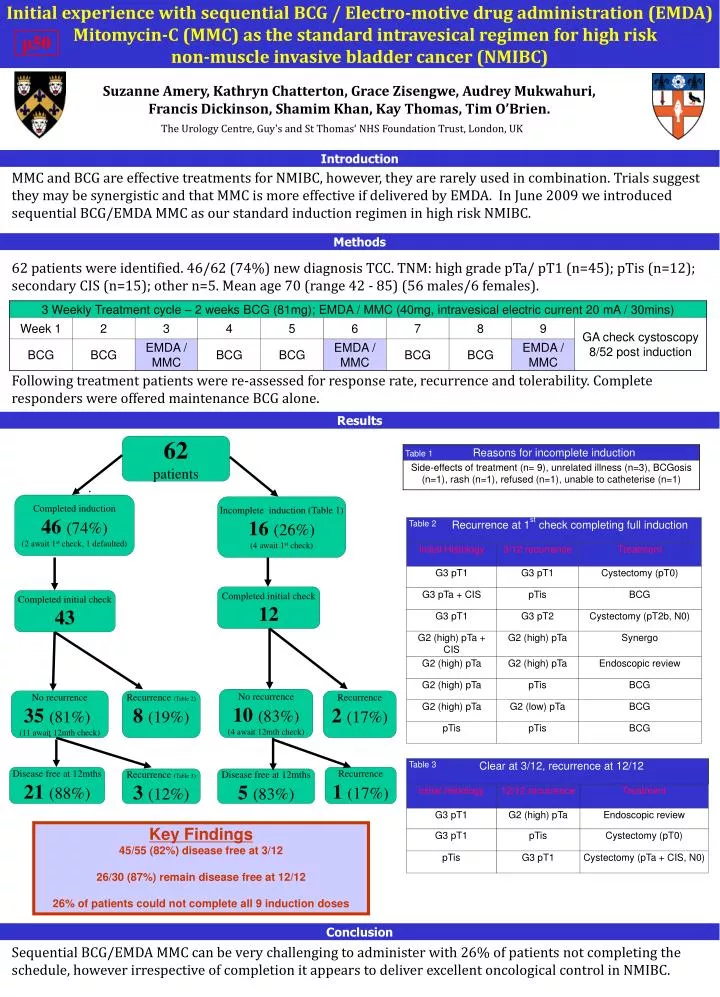
Initial experience with sequential BCG / Electro-motive drug administration (EMDA) Mitomycin-C (MMC) as the standard intravesical regimen for high risk non-muscle invasive bladder cancer (NMIBC) p50 Suzanne Amery, Kathryn Chatterton, Grace Zisengwe, Audrey Mukwahuri, Francis Dickinson, Shamim Khan, Kay Thomas, Tim O’Brien. The Urology Centre, Guy's and St Thomas‘ NHS Foundation Trust, London, UK Introduction MMC and BCG are effective treatments for NMIBC, however, they are rarely used in combination. Trials suggest they may be synergistic and that MMC is more effective if delivered by EMDA. In June 2009 we introduced sequential BCG/EMDA MMC as our standard induction regimen in high risk NMIBC. Methods 62 patients were identified. 46/62 (74%) new diagnosis TCC. TNM: high grade pTa/ pT1 (n=45); pTis (n=12); secondary CIS (n=15); other n=5. Mean age 70 (range 42 - 85) (56 males/6 females). Following treatment patients were re-assessed for response rate, recurrence and tolerability. Complete responders were offered maintenance BCG alone. Results 62 patients Completed induction 46(74%) (2 await 1st check, 1 defaulted) Incomplete induction (Table 1) 16(26%) (4 await 1st check) Completed initial check 12 Completed initial check 43 No recurrence 10(83%) (4 await 12mth check) No recurrence 35(81%) (11 await 12mth check) Recurrence (Table 2) 8(19%) Recurrence 2(17%) Disease free at 12mths 21(88%) Recurrence 1(17%) Recurrence (Table 3) 3(12%) Disease free at 12mths 5(83%) Key Findings 45/55 (82%) disease free at 3/12 26/30 (87%) remain disease free at 12/12 26% of patients could not complete all 9 induction doses Conclusion Sequential BCG/EMDA MMC can be very challenging to administer with 26% of patients not completing the schedule, however irrespective of completion it appears to deliver excellent oncological control in NMIBC.