Download
1 / 32
370 likes | 1.59k Views
Endometrial Cancer. Brought to you by: Kathryn Bezzina and LL Chepelev. Objectives. 4392 : List the risk factors for endometrial carcinoma . 4393 : Describe the important pathologic features of endometrial carcinoma which predict prognosis .

E N D
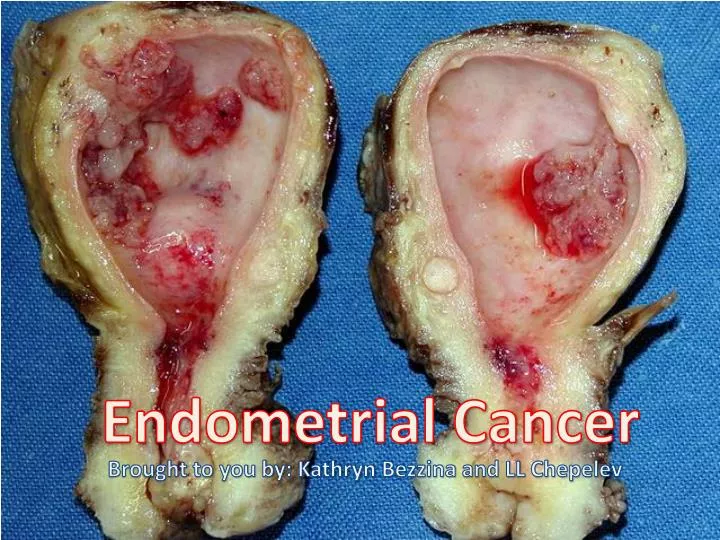
Endometrial Cancer Brought to you by: Kathryn Bezzina and LL Chepelev
Objectives 4392: List the risk factors for endometrial carcinoma. 4393: Describe the important pathologic features of endometrialcarcinoma which predict prognosis. • DDxof Post-menopausal Bleeding and Necessary Investigations • List Risk Factors for Endometrial Cancer • Types of Endometrial Cancer • Management Principles – Surgical Staging • Describe how histology and stage affect prognosis
Endometrial Carcinoma: Epidemiology #1 gynecological malignancy in North America (40%) • 4th most common cancer in women 2-3% of women develop endometrial carcinoma during lifetime Mean age is 60 years, with peak incidence in 7th decade • 25% are diagnosed in premenopausal women • 75% are postmenopausal Majority with early diagnosis due to symptom detection • 85-90% 5-yr survival for Stage I disease • 70-80%overall 5-yr survival for all stages • HIGHEST CURE RATE of gynecological CA
Endometrial Cancer RiskFactors COLD NUT Cancer (Ovarian, Breast, Colon) Obesity Late Menopause Diabetes Mellitus Nulliparity Unopposed Estrogen (PCOS, Anovulation, HRT) Tamoxifen: Chronic Use
Presentation, Signs & Symptoms Postmenopausal bleeding = Endometrial CA UPO lesion Bx 95% Px w vaginal bleeding
Postmenopausal Bleeding: DDx • Atrophy (60%) – irregular sloughing of the cells • Polyps (12%) • Endometrial cancer (10%) • Endometrial Hyperplasia (10%) • Simple Complex Cancerous • Hormonal effect (7%) • Cervical Cancer (<1%) • Other (eg. Hematometra, trauma, etc.) Postmenopausal bleeding = Endometrial CA UPO lesion Bx 95% Px w vaginal bleeding
Workup for Post-Menopausal Bleeding PEx • Calculate BMI • Speculum examination • Rectovaginalexamination Investigations • Endometrial biopsy as the INITIAL DIAGNOSTIC TEST • or D&C • Cervical CA screening Hx • When did bleeding start? • Were there precipitating factors (trauma)? • What is the nature of the bleeding (temporal pattern, duration, post-coital [cervical CA], quantity) • Sx: fever, pain, changes in bowel/bladder function? • PMHx, Meds (hormones, anticoagulants, tamoxifen) • FHx: endometrial, breast, colon, CA?
Prognostic Factors • FIGO Stage • Tumor Histological Grade • Histopathologic Type • Progesterone Receptor Levels (i.e. Type I or Type II) • Myometrial Invasion • Lymphovascular Space Invasion • Lymph Node Involvement • Lower Uterus Involvement • Age • Tumor Remnants after Surgery • Race: better prognosis and more Type 1 in Caucasians over Blacks • Molecular Markers
Histological Grade Well-Differentiated Cells Intermediate Grade Poorly-Differentiated Cells
FIGO Staging Stage I Above Stage I
Therapy OptionsIt Depends • Surgery when staging would be extended to mass excision. • Exploratory laparotomy • Total abdominal hysterectomy • Bilateral salpingo-oophorectomy • Peritoneal cytology • Pelvic and para-aortic lymphadenectomy • Medications: Cisplatin • Radiotherapy
Adjuvant Therapy • Low Risk + Fertility: Progestin • Low-Intermediate: Observation • High-Intermediate: Radiation Therapy, Vaginal Brachytherapy • High: Chemotherapy +/- RT • Post-Treatment Surveillance
Case A 66 yo nulliparous woman who underwent menopause at age 55 years complains of a 2-week history of vaginal bleeding. Prior to menopause, she had irregular menses. She denies use of hormone therapy. Her medical history is significant for diabetes mellitus controlled with an oral hypoglycemic agent. On examination, she weighs 100 kg and is 172 cm in height. Her blood pressure is 150/90 and temperature 37.5 degree Celcius. Heart and lung examination is normal. Abdomen is obese, no masses palpable. The external genitalia appear normal, and the uterus seems to be of normal size without any demonstrable pelvic mass.