Download
1 / 55
720 likes | 2.47k Views
Disorders of Sebaceous Glands. Prof. Ashraf Al-Sawy MD. The sebaceous gland. Found at great abundance on face and scalp. Distributed any where except palms and soles. Seb . Gland consits of many lobes and duct which opens into a hair follicle ( pilosebaceous unit).

E N D
Disorders of Sebaceous Glands Prof. Ashraf Al-Sawy MD.
Found at great abundance on face and scalp. • Distributed any where except palms and soles.
Seb. Gland consits of many lobes and duct which opens into a hair follicle (pilosebaceous unit).
Starts their activity after puberty. • They are under androgenic control. • Functions of sebum: • Moisturizing the skin. • Protects the skin against fungal and bacterial infection.
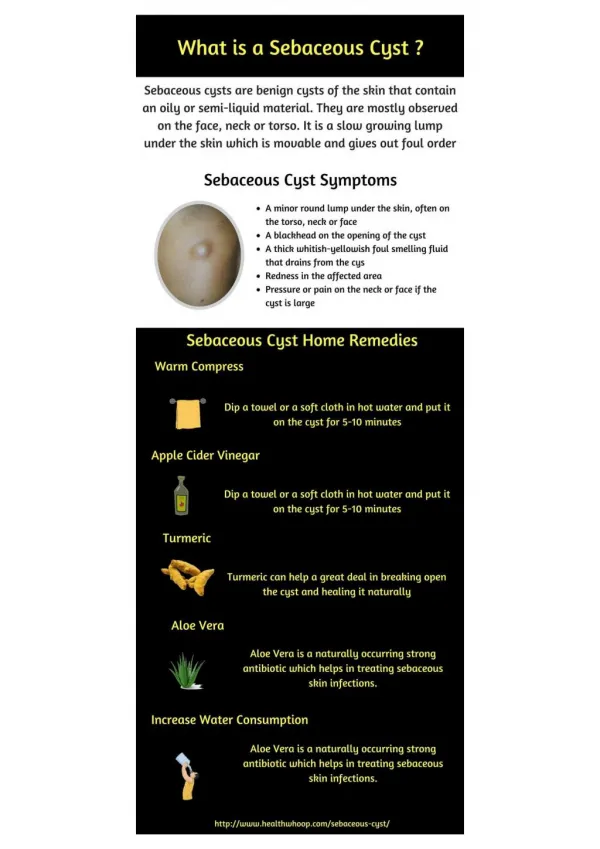
Definition • A multifacorial disorder of the pilosebaceous apparatus. • Affects 85-100% of people. • Characterized by • Papules: • Non-inflammatory (comedones). • Inflammatory. • Pustules. • Nodules. • Cysts.
Distribution • Affects the areas of skin with the densest population of sebaceous follicles: • Face. • The upper part of the chest. • The back. • Meles & females are equally affected
Pathogenesis • Multifactorial disease resulting from: • 1) Excessive sebum production. • 2) Follicular epidermal hyperproliferaion and hyperkeratinization with resultant accumulation of keratin and sebaceous debris • 3) Proliferation of bacteria in the pilosebaceous unit • 4)Inflammation.
Increased activity of sebaceous glands and occlusion of the cornfied hypertrophic pilosebaceous follicles lead to retention of sebum into the follicles, which dilate and rupture by time. • Abnormal flora (propioniform bacterium acnes) and anaerobes such as Corynebacterium acne, Pityrosporom ovale and Staphylococci cause split of the sebum into fatty acids and triglycerides which act as an important irritating factors . • This will lead to the formation of the different clinical lesions (polymorphic) of acne which varies from papules, pustules ,cysts and comedones.
Genetic Factors • More than one member of the family is affected. • Influence the development of lesions. • Influence the course and severity of the disease.
Hormones • Androgens Stimulate the activity of sebaeous glands with increased sebum production. • Estrogen has inhibitory effect.
Ductal Hypercornification • Leads to occlusion of the pilosebaceous follicles that lead to retention of sebum into the follicles, which dilate and rupture by time.
P. acnes • Splitting of sebum into free fatty acids and triglycerides • Which are irrtants and cause inflammation
Mediators of inflammation • Inflammation is due to the biologically active mediators rather than the direct bacterial infection.
Factors which aggravate acne • Menstruation: • 70% of women complain of a flare 2-7 days premenstrually. • Stress • Sweating: 15% of patients notice that sweating deteriorates acne. • Genetic factors. • Cosmetics & hair pomade. • Medications: iodides, antiepileptics, stroides. • Congenital adrenal hyperplasia, PCO.
Lines of treatment: • Topical treatment. • Systemic Treatment: • Antibiotics. • Antiandrogens. • Retinoids. • Sytemic steriods. • Physical modalities. • Treatment of post-acne scars & hyperpigmentation.
Predominantly inflammatory lesions : • Benzoyl peroxide • Topical antibiotics: clindamycin, erythromycin or erythromycin + Zn acetate 1.2% • Azelaic acid 20% • Adapalene • Predominantly non-inflammatory lesions (anticomedonal): • Retinoic acid 0.05% • Isotretinoin 0.05% • Adapalene • Azelaic acid
Topical antibiotic products • Clindamycin • Solution, gel, lotion, pledget and foam: 1%. • Erythromycin • Solution, gel, cream, pledget: 1.5% or 2%.
Benzoyl Peroxide 5-10% • Bacteriostatic. • It has peeling effect. • Comedolytic. • Its disadvantages are: • slight irritation. • bleaching of clothes.
Systemic Antibiotics • Duration: at least 6 months, but changed at 3 months if not successful. • Mechanism of action of antibiotics: inhibition of P. acnes lipases and chemotactic substances, complement pathway and neutrophil migration.
Tetracyclines: • (1 gm daily) better on an empty stomach. • It is contraindicated in pregnancy, hepatic & renal impairement. • Minocycline: • 100 mg/d • Erythromycin: • (1 gm daily) especially in women who might become pregnant.
Clindamycin (Dalacine C®): • 150 mg, 3 times daily. • Risk of colitis. • Doxycycline (Vibramycin®): • 100 mg daily. • Trimethoprim - sulfamethoxazole (Septrim®): 400-600 mg/day.
Hormonal Therapy • Oral contraceptives: • Estrogen • Antiandrogens: • Ethinylestradiol + cyproterone acetate • Used only in non-pregnant females.
Oral contraceptives Therapeutic effects Side effects Nausea Irregular menses Weight gain / bloating Increased risk blood clots Hypertension Decreases ovarian androgens Decreases free testosterone Decreases sebum production Decreases inflammatory lesions Layton AM. Am Clin J Dermatol 2: 135-141, 2001. Krowchuk DP, Lucky AW. Adolsec Med 12: 355-374, 2001.
Oral Retinoids • (Isotretinoin, 13-Cis-retinoic acid • Accutane® - Roaccutane®” • 1 mg/kg/day for 4-5 months) • Make sure that females with acne are not pregnant before you put them on isotretinoin, and that they do not become pregnant during the course and for 1-3 months after it.
Indications: • Severe acne: nodulocystic acne, severe inflammatory acne with scarring. • Moderate acne not responding to, or relapsed after, conventional combined oral & topical antibiotics for 6 months. • Severe psychological distress.
Dose: 0.5-1 mg/kg for 4-5 months. • Intermittent moderate dose (0.5 mg/kg/day taken/week out of 4 weeks for a total of 6 months) is effective in mature adults with persistent and late-onset acne.
Comedo extraction • Intralesional injection of steroides. • Cryotherapy.