Download
1 / 30
320 likes | 538 Views
NQF-endorsed™ Safe Practices for Better Healthcare. Safe Practice 7 Disclosure. Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver. Slide Deck Overview. Slide Set Includes:

E N D
NQF-endorsed™ Safe Practices for Better Healthcare Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
Slide Deck Overview Slide Set Includes: • Section 1: NQF-endorsed™ Safe Practices for Better Healthcare Overview • Section 2: Harmonization Partners • Section 3: The Problem • Section 4: Practice Specifications • Section 5: Example Implementation Approaches • Section 6: Front-line Success Stories
NQF-endorsed™ Safe Practices for Better Healthcare Overview Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
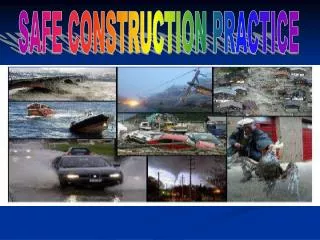
2010 NQF Safe Practices for Better Healthcare: A Consensus Report • 34 Safe Practices • Criteria for Inclusion • Specificity • Benefit • Evidence of Effectiveness • Generalization • Readiness
Culture SP 1 2010 NQF Report
Culture • CHAPTER 2: Creating and Sustaining a Culture of Patient Safety (Separated into Practices] • Leadership Structures and Systems • Culture Measurement, Feedback, and Interventions • Teamwork Training and Team Interventions • Identification and Mitigation of Risks and Hazards Structures and Systems Culture Meas., FB., and Interv. Team Training and Team Interv. ID and Mitigation Risk and Hazards Consent & Disclosure Consent and Disclosure • CHAPTER 3: Informed Consent and Disclosure • Informed Consent • Life-Sustaining Treatment • Disclosure • Care of the Caregiver Informed Consent Life-Sustaining Treatment Disclosure Care of Caregiver Workforce • CHAPTER 4: Workforce • Nursing Workforce • Direct Caregivers • ICU Care Nursing Workforce Direct Caregivers ICU Care • CHAPTER 5: Information Management and Continuity of Care • Patient Care Information • Order Read-Back and Abbreviations • Labeling Studies • Discharge Systems • Safe Adoption of Integrated Clinical Systems including CPOE Information Management and Continuity of Care Patient Care Info. Read-Back & Abbrev. Labeling Studies Discharge System CPOE Medication Management • CHAPTER 6: Medication Management • Medication Reconciliation • Pharmacist Leadership Role Including: High-Alert Med. and Unit-Dose Standardized Medication Labeling and Packaging Med. Recon. Pharmacist Systems Leadership: High-Alert, Std. Labeling/Pkg., and Unit-Dose • CHAPTER 7: Hospital-Associated Infections • Hand Hygiene • Influenza Prevention • Central Venous Catheter-Related Blood Stream Infection Prevention • Surgical-Site Infection Prevention • Care of the Ventilated Patient and VAP • MDRO Prevention • UTI Prevention Healthcare-Associated Infections Hand Hygiene Influenza Prevention Central V. Cath. BSI Prevention Sx-Site Inf. Prevention VAP Prevention MDRO Prevention UTI Prevention • CHAPTER 8: • Wrong-Site, Wrong-Procedure, Wrong-Person Surgery Prevention • Pressure Ulcer Prevention • DVT/VTE Prevention • Anticoagulation Therapy • Contrast Media-Induced Renal Failure Prevention • Organ Donation • Glycemic Control • Falls Prevention • Pediatric Imaging Condition-, Site-, and Risk-Specific Practices Wrong-site Sx Prevention Press. Ulcer Prevention DVT/VTE Prevention Anticoag. Therapy Contrast Media Use Organ Donation Glycemic Control Falls Prevention Pediatric Imaging
Harmonization Partners Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
The Objective Disclosure • Provide open and clear communication with patients and their families about serious unanticipated outcomes that is supported by systems that foster transparency and performance improvement to reduce preventable harm.
The Problem Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
The Problem Frequency • 40% of the American public have reported a medical error in their own care or a family member’s care • Research has shown that disclosure happens once in every four harmful events [Blendon, N Engl J Med 2002 Dec 12;347(24):1933-40; Denham, J Patient Saf 2006 Dec;2(4):225-32; Sheridan, J Patient Saf 2008 Mar;4(1):18-26]
The Problem Severity • One report suggested that one out of four medical errors results in death, disability, or severe pain • Serious preventable harm causes emotional trauma for patients and families • However, when these incidents occur, clinicians often overlook disclosure in fear of the implications of liability [Blendon, N Engl J Med 2002 Dec 12;347(24):1933-40; Leape, Physician Exec. 2006 Mar-Apr;32(2):16-8; Gallagher, Arch Intern Med 2006 Aug 14-28;166(15):1585-93; Gallagher, Arch Intern Med 2006 Aug 14-28;166(15):1605-11; Denham, J Patient Saf 2006 Sep;2(3):162-70; Denham, J Patient Saf 2008 Jun;4(2):119-23]
The Problem Preventability • Implement full disclosure programs that include the caregiver, who acknowledges the error, takes responsibility, and apologizes • The process of disclosure must include the concerned caregivers • Organizations must provide the necessary support systems to assist patients and caregivers throughout the process [Denham, J Patient Saf 2007 Jun;3(2):107-19: Iedema, Int J Qual Health Care 2008 Dec;20(6):421-32; Holden, BMJ 2009 Feb 10;338:b520; Wu, J Gen Intern Med 2009 Jul 4]
The Problem Cost Impact • University of Michigan experienced $2 million annual savings from a full disclosure policy • The Lexington Veterans Affairs Medical Center reported an average settlement payout of $82K less than the national Department of Veterans Affairs average, due to their disclosure policy [Kraman, Jt Comm J Qual Improv 2002 Dec;28(12):646-50; Clinton, N Engl J Med 2006 May 25;354(21):2205-8; Wojcieszak, Jt Comm J Qual Patient Saf 2006 Jun;32(6):344-50; McDonald, Responding to Patient Safety Incidents: The Seven Pillars, 2009]
Practice Specifications Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
Safe Practice Statement Disclosure • Following serious unanticipated outcomes, including those that are clearly caused by systems failures, the patient and, as appropriate, the family should receive timely, transparent, and clear communication concerning what is known about the event [MCPME, When Things Go Wrong: Responding to Adverse Events, 2006; UMich, Patient Safety Toolkit – Disclosure Chapter, 2009; Institute for Healthcare Improvement, Communication with Patients and Families after an Adverse Event. IHI Improvement Map, 2009]
Additional Specifications • Serious unanticipated outcomes include sentinel events, serious reportable events, and outcomes requiring substantial additional care • Create formal processes for disclosing unanticipated outcomes and for reporting events to those responsible for patient safety • Policies should incorporate continuous quality improvement techniques and provide for annual reviews and updates • Adherence to the practice and participation with the support system are expected [NQF, Serious Reportable Events in Healthcare: A Consensus Report, 2002; Kussman, Disclosure of adverse events to patients, 2008; Sorenson, 2008; TJC, J Health Serv Res Policy 2008 Oct;13(4):227-32, 2009; JCR, 2010 Comprehensive Accreditation Manual: CAMH for Hospitals: The Official Handbook, 2010]
Additional Specifications • Patient communication should be characterized by sharing the facts, showing empathy, and giving an apology • Implement a procedure to ensure and document that all LIPs are provided with a detailed description of the organization’s program for responding to adverse events • Implement a process that will provide information to a Patient Safety Organization that would protect confidential information • Create a process that will allow a patient to waive medical billing in the case of systemic or human error [Agency for Healthcare Research and Quality, Legislation and Regulations: Patient Safety and Quality Improvement Act of 2005 (the Patient Safety Act): An Overview; Fein, J Gen Intern Med 2007 Jun;22(6):755-61; Iedema, Int J Qual Health Care 2008 Dec;20(6):421-32; Holden, BMJ 2009 Feb 10;338:b520 ]
Example Implementation Approaches Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
Example Implementation Approaches • Implement procedures that incorporate critical practice elements and provide healthcare workers with disclosure education and just-in-time coaching • Establish processes to comply with this practice through the collaborative work of governing boards, senior administrative leaders, medical staff, and risk management leaders • Start with simple processes, basic educational strategies, and clear engagement tactics that incorporate the practice into existing meetings to ensure it becomes a part of the way an organization operates [Camiré, CMAJ 2009 Apr 28;180(9):936-43; Gunderson, An International Journal 2009; 21(3):229-32]
Example Implementation Approaches Strategies of Progressive Organizations • Some organizations are experimenting with policies that involve disclosing a broader range of unanticipated outcomes • High-performing organizations are tracking waived costs generated because of adverse events and are allocating accountabilities to departments and care providers • Leading academic organizations are teaching disclosure to nursing and medical students [McDonald, "Full Disclosure" and Residency Education, 2008; McDonald, Responding to Patient Safety Incidents: The Seven Pillars, 2009]
Front-line Success Stories Safe Practice 7 Disclosure Chapter 3: Improving Patient Safety Through Informed Consent, Life-Sustaining Treatment, Disclosure, and Care of the Caregiver
Title of Video Insert Video this size
TMIT High Performer Webinar Creating Transparency, Openness, and Improved Safety (Safe Practices 5-8) • This webinar will cover the importance of policies for caring for those who provide care, and how to improve patient safety through informed consent, life-sustaining treatment, and disclosure • Go to: http://www.safetyleaders.org/pages/idPage.jsp?ID=4972
TMIT High Performer Webinar Consent, End of Life, and Disclosure • Renowned educators and subject matter experts Tom Gallagher, MD, Lee Taft, JD, and Gail Nielsen, in the fields of informed consent, life-sustaining treatments, disclosure practices, and healthcare literacy, will guide you in special informational sessions about the importance and implementation of these revised and new Safe Practices. Jennifer Dingman, a national patient safety advocate, will provide the patient and family perspective. • Go to: http://www.safetyleaders.org/pages/idPage.jsp?ID=4687