Download
1 / 21
400 likes | 1.05k Views
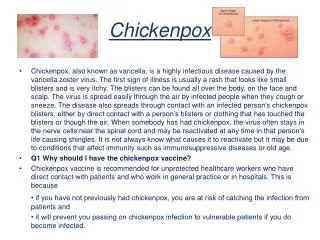
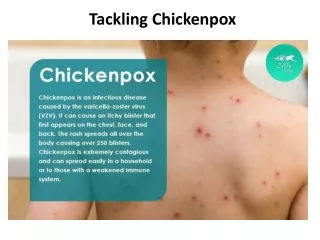
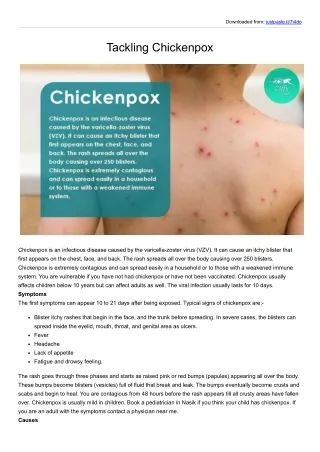
Chickenpox . Varicella Zoster. Highly contagious. Most people infected by age 5. Immunity increases with age. Outbreaks usually winter/ spring. Epidemics every 2-5 yrs. Spreads via respiratory tract. Incubation 10-14 days (up to 21).

E N D
Varicella Zoster. • Highly contagious. • Most people infected by age 5. • Immunity increases with age. • Outbreaks usually winter/ spring. • Epidemics every 2-5 yrs.
Spreads via respiratory tract. • Incubation 10-14 days (up to 21). • Infective from 4 days before rash, until crusts fall off. • Days 1 & 2 most infective.
Presentation • Infection & immunity may occur without clinical disease • Pyrexia for up to 4/7 (38-39⁰C) • Headache • Malaise • Abdo pain • Dry cough • Sore throat • Itchy rash
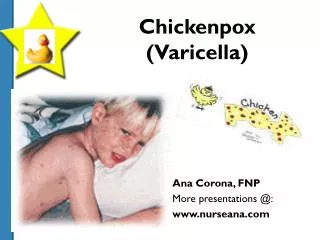
Rash • Crops of vesicles appear over 3-5 days. • Usually head, neck & trunk (sparse on limbs). • Can involve vulva, mouth, oropharynx. • Papule → vesicle→ pustule → crust. • Crusts fall off leaving mark, (last few wks). • Usually no long term scarring.
← Early rash Excoriation→
Usually mild-moderate • Self-limiting • Risk factors for complications; • Older age • Immunocompromised • Long term steroids (>2mg day>14/7 child) (>40mg day >1/52 adult) • Pregnancy • Malignancy
Complications • 2⁰ Infection (scratching). • 2⁰ Bacterial infection esp. Group A Strep. →TSS & Necrotising fasciitis. • Encephalitis. • CNS – cerebellar ataxia, myelitis, vasculititis→CVA. • Osteomyelitis, sepsis, otitis media.
Management in Healthy • Fluids • Antipyretics • Antihistamines • Abx for 2⁰ infection • Avoid pregnant women, neonates, immunocompromised. • Acyclovir if <24 hrs & risk of complications.
Antiviral Treatment • Oral Acyclovir – Adults 800mg 5 x daily - Children 20mg/Kg x 4 daily • Chronic medical condition • >12 yrs to reduce complication rate • 2nd case in a household • Pregnant (not licensed, no evidence of teratogenicity) • Consider IV (immunocomp., systemic disease, steroids, new lesions> 8/7)
IV Acyclovir • High risk immunocompromised; • Haematological malignancy • HIV CD4 <200 cells/mm3 • Organ transplant • High dose immunosuppressive therapy • Systemic heart or lung disease • High dose steroids • New lesions appearing after 8/7
Varicella Contact • Face-face >4 hrs • Oral acyclovir • No previous exposure • Serological testing to confirm (need results within 2/7) • 5-7/7 post-exposure • Pt high risk/ transmission to high risk (child is immunocomp)
Varicella in Pregnancy • If previous exposure, then no risk. • Ideally serological testing to confirm previous exposure. • High risk <96hrs after exposure →VZIG. • Antivirals if >96hrs • Specialist advice re; confirmation & fetal varicella syndrome. • No correlation between severity of chickenpox and risk to foetus.
Complication risk ↑,esp Maternally e.g. pneumonia. • <20/40 2% risk of congenital varicella syndrome. • >20/40 risk of preterm birth or neonatal herpes zoster. • 1st yr of life, usually affecting thoracic dermatome. • Rash appears 7/7 prior to delivery – 2/7 after • Neonatal infection • IgM (initial response) doesn’t cross placenta • 30% risk of death from pneumonia/hepatitis • IV acyclovir & immunoglobulin • Rash > 1/52 after delivery IgG should give adequate protection.
MolluscumContagiosum • Molluscum contagiosum virus. • DNA pox virus. • 4 types, MCV1 causes most. • Spreads via direct skin contact; • Contact sports • Sharing baths/ towels • Gym equipment • Common (↑ immunocompromised).
Incubation period 2-7 weeks. • Usually asymptomatic. • May be redness, irritation or eczema around the lesions.
Examination • Firm, smooth, umbilicated papules. • 2-6mm diameter. • Present in groups or spread. • Skin colour, white, translucent or yellowy in colour. • 1-20 lesions but may be more. • Any one lesion is likely to last approx. 2 months.
Management • No school exclusion. • Self – limiting. • Settles in 12-18 months. • Management usually nothing – esp. in children. • Adults - Liquid nitrogen - Imiquimod - Pierce lesions with sterile needle