Download
1 / 64
780 likes | 1.38k Views
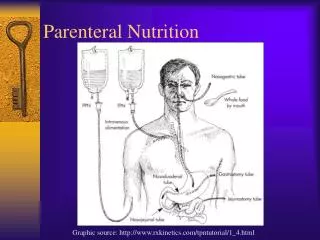
Chapter 23. Enteral and Parenteral Nutrition Support. Enteral Nutrition Definition. Nutritional support via placement through the nose, esophagus, stomach, or intestines (duodenum or jejunum) —Tube feedings —Must have functioning GI tract —IF THE GUT WORKS, USE IT!

E N D
Chapter 23 Enteral and Parenteral Nutrition Support
Enteral Nutrition Definition • Nutritional support via placement through the nose, esophagus, stomach, or intestines (duodenum or jejunum) —Tube feedings —Must have functioning GI tract —IF THE GUT WORKS, USE IT! —Exhaust all oral diet methods first.
Oral Supplements • Between meals • Added to foods • Added into liquids for medication pass by nursing • Enhances otherwise poor intake • May be needed by children or teens to support growth
Conditions That Require OtherNutrition Support • Enteral —Impaired ingestion —Inability to consume adequate nutrition orally —Impaired digestion, absorption, metabolism —Severe wasting or depressed growth • Parenteral —Gastrointestinal incompetency —Hypermetabolic state with poor enteral tolerance or accessibility
Algorithm for Decisions Modified and adapted from Gorman RC, Morris JB: Minimally invasive access to the gastrointestinal tract. In Rombeau JL, Rolandelli RH, editors: Clinical nutrition: enteral and tube feeding, p 174, Philadelphia, 1997, WB Saunders; and Ali A et al: Nutritional support services, Nutritional Support Algorithms, 8(7):13, July 1998.
Considerations in Enteral Nutrition • Applicable • Site placement • Formula selection • Nutritional/medical requirements • Rate and method of delivery • Tolerance
Formula Selection • Functional status of GI tract • Physical characteristics of formula (osmolality, fiber content, caloric density, viscosity) • Macronutrient ratios • Digestion and absorption capability of patient • Specific metabolic needs • Contribution of the feeding to fluid and electrolyte needs or restriction • Cost effectiveness The suitability of a feeding formula should be evaluated based on
Enteral Access: Clinical Considerations • Duration of tube feeding —Nasogastric or nasoenteric tube for short term —Gastrostomy and jejunostomy tubes for long term • Placement of tube —Gastric —Small bowel
Placement Site • Access (medical status) • Location (radiographic confirmation) • Duration • Tube measurements and durability • Adequacy of GI functioning
Advantages—Enteral Nutrition • Intake easily/accurately monitored • Provides nutrition when oral is not possible or adequate • Costs less than parenteral nutrition • Supplies readily available • Reduces risks associated with disease state
More Advantages—Enteral Nutrition • Preserves gut integrity • Decreases likelihood of bacterial translocation • Preserves immunologic function of gut • Increased compliance with intake
Disadvantages—Enteral Nutrition • GI, metabolic, and mechanical complications—tube migration; increased risk of bacterial contamination; tube obstruction; pneumothorax • Costs more than oral diets • Less “palatable/normal” • Labor-intensive assessment, administration, tube patency and site care, monitoring
Complications of Enteral Feeding • Access problems (tube obstruction) • Administration problems (aspiration) • Gastrointestinal complications (diarrhea) • Metabolic complications (overhydration)
Aspiration Pneumonia • Can result from enteral feeds • High-risk patients —Poor gag reflex —Depressed mental status
Reducing Risk of Aspiration • Check gastric residuals if receiving gastric feeds • Elevate head of the bed >30 degrees during feedings • Postpyloric feeding —Nasoenteric tube placement may require fluoroscopic visualization or endoscopic guidance —Transgastric jejunostomy tube
Rate and Method of Delivery* • Bolus—300 to 400 ml rapid delivery via syringe several times daily • Intermittent─300 to 400 ml, 20 to 30 minutes, several times/day via gravity drip or syringe • Cyclic—via pump usually at night • Continuous—via gravity drip or infusion pump *Determined by medical status, feeding route and volume, and nutritional goals
Consideration of Physical Properties of Enteral Formulas • Residue • Viscosity —Size of tube is important • Osmolality: consider protein source —Intact (do not affect osmolality)—soy isolates; sodium or calcium casein; lactalbumin —Hydrolyzed (more particles)—peptides or free amino acids
Renal Solute Load • Normal adult tolerance is 1200 to 1400 mOsm/L • Infants and renal patients may tolerate less
Lower Osmolality • Large (intact) proteins • Large starch molecules
Higher Osmolality • Hydrolyzed protein or amino acids • Disaccharides
Tolerance • Signs and symptoms: —Consciousness —Respiratory distress —Nausea, vomiting, diarrhea —Constipation, cramps —Aspiration —Abdominal distention
Tolerance—cont’d • Other signs and symptoms —Hydration —Labs —Weight change —Esophageal reflux —Lactose/gluten intolerances —Glucose fluctuations
How to Determine Energy and Protein kcal/ml x ml given = kcal % protein x kcal = kcal as protein kcal as protein x 1 g/4 kcal = g protein Example: Patient drinks 200 cc of a 15.3% protein product that has 1 kcal/ml 1 kcal/ml x 200 ml = 200 kcal 0.153 % protein x 200 kcal = 30.6 kcal 30.6 kcal x 1g protein/4 kcal = 7.65 g protein
Energy in Formulas 1 to 1.2 kcal/ml = usual concentration 2 kcal/ml = highest concentration
Protein • From 4% to 26% of kcal is possible • 14% to 16% of kcal is usual • 18% to 26% of kcal—considered to be high-protein solution
Recommended Water • Healthy adult: 1 ml/kcal or 35 ml/kg • Healthy infant: 1.5 ml/kcal or 150 ml/kg • Normal tube feeding: 1 kcal/ml; 80% to 85% water • Elderly: consider 25 ml/kg with renal, liver, or cardiac failure; or consider 35 ml/kg if history of dehydration
Sources of Fluid (“Free Water”) • Liquids • Water in food • Water from metabolism • With tube feeding, nurse will flush tube with water about 3 times daily—include this amount in estimated needs —Example: “flush with 200 cc tid”
Administration: Feeding Rate • Continuous method = slow rate of 50 to 150 ml/hr for 12 to 24 hours • Intermittent method = 250 to 400 ml of feeding given in 5 to 8 feedings per 24 hours • Bolus method = may give 300 to 400 ml several time a day (“push” is not desired)
French Units—Tube Size • Diameter of feeding tube is measured in French units • 1F = 33 mm diameter • Feeding tube sizes differ for formula types and administration techniques.
Examples of Special Formulas • Pediatrics • Low residue • High protein • Volume restriction • Diabetic • Pulmonary/COPD
Routes of Parenteral Nutrition • Central access —TPN both long- and short-term placement • Peripheral or PPN —New catheters allow longer support via this method limited to 800 to 900 mOsm/kg due to thrombophlebitis <2000 kcal required or <10 days
PPN vs. TPN • Kcal required(10% dextrose max. PPN conc.) • Fluid tolerance • Osmolarity • Duration • Central line contraindicated
Venous Sites from Which the Superior Vena Cava May Be Accessed
Advantages—Parenteral Nutrition • Provides nutrients when less than 2 to 3 feet of small intestine remains • Allows nutrition support when GI intolerance prevents oral or enteral support
Indications for Total Parenteral Nutrition • GI non functioning • NPO >5 days • GI fistula • Acute pancreatitis • Short bowel syndrome • Malnutrition with >10% to 15 % weight loss • Nutritional needs not met; patient refuses food
Contraindications • GI tract works • Terminally ill • Only needed briefly (<14 days)
Calculating Nutrient Needs • Avoid excess kcal (> 40 kcal/kg) • Adults kcal/kg BW Obese—use desired BMI range or an adjusted factor
Adjusted Body Weight Adjusted IBW for obesity Female: ([actual weight – IBW] x 0.32) + IBW Male: ([actual weight – IBW] x 0.38) + IBW
Parenteral Components • Carbohydrate glucose or dextrose monohydrate 3.4 kcal/g • Amino acids 3, 3.5, 5, 7, 8.5, 10% solutions • Fat 10% emulsions = 1.1 kcal/ml 20% emulsions = 2 kcal/ml
Protein Requirements • 1.2 to 1.5 g protein/kg IBW mild or moderate stress • 2.5 g protein/kg IBW burns or severe trauma
Carbohydrate Requirements • Max. 0.36 g/kg BW/hr • Excess glucose causes: Increased minute ventilation Increased CO2 production Increased RQ Increased O2 consumption Lipogenesis and liver problems
Lipid Requirements • 4% to 10% kcals given as lipid meets EFA requirements; or 2% to 4% kcals given as lineoleic acid • Usual range 25% to 35% max. 60% of kcal or 2.5 g fat/kg
Other Requirements • Fluid—30 to 50 ml/kg • Electrolytes Use acetate or chloride forms to manage acidosis or alkalosis • Vitamins • Trace elements