Download
1 / 111
1.15k likes | 1.68k Views
CT Scans of the Head: A Neurologist’s Perspective . Lara Cooke January 15, 2009. Objectives. At the end of this session, residents should be able to: Identify key anatomic structures on CT Apply an approach to reading a CT of the head List reasons to image a patient with headache

E N D
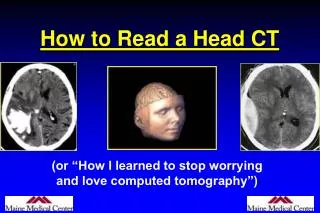
CT Scans of the Head:A Neurologist’s Perspective Lara Cooke January 15, 2009
Objectives • At the end of this session, residents should be able to: • Identify key anatomic structures on CT • Apply an approach to reading a CT of the head • List reasons to image a patient with headache • Identify CT signs of raised ICP, early ischemia • Describe the clinical presentation of dural sinus thrombosis • Distinguish between intracranial hemorrhages
General Principles of the CT • CT is basically a specialized X-Ray • We talk about “density” or “attenuation” • The image is a measure of absorption of X-rays through different angles through a given tissue and then transformed mathematically
What is hyperdense vs hypodense on CT? • Bone (dense calcium) (1000 HU) • Metal • Acute (but not hyperacute) blood (56-76 HU) • Thrombosis • Grey matter>white matter (30, 20 HU) • CSF (0 HU) • Fat (-30-100 HU) • Air (-1000)
General Principles: • Are there any fractures? • Use bone windows • Look around the orbits, skull base, zygoma • Remember to look at the sinuses (frontal, maxillary, ethmoid, sphenoid, mastoid air cells) • Should be black & full of air--look for hyperdense fluid levels, thickening of mucosa, cysts….especially when the patient complains of headache
Bones Fracture
Sinuses Maxillary Sphenoid Frontal Ethmoid
General Principles • Look at the dura • Is there anything ‘extra’ between the brain and the skull? • Hygroma • Blood • Tumor • Air
Things between skull & brain that shouldn’t be there Hygroma Meningioma Subdural hematoma Epidural hematoma Pneumocephaly
General Principles • Look at the brain: • Grey-white differentiation • Basal ganglia • Internal capsule • Corona radiata • Is there blood? Is there edema? Is there CSF due to encephalomalacia/cysts? Is there a mass?
GW DifferentiationAnatomic Structures Anterior horn of lateral ventricle caudate lentiform Internal capsule (post. limb) Insular ribbon Sylvian fissure Pineal gland thalamus 3rd ventricle
General Principles • Look at the spaces • Ventricles: • Can you see all the ventricles? • Is there hydrocephalus? • Cisterns • Are the normal spaces around the brainstem still visible? • Dural Sinuses • Can you see them? • Are they thicker or brighter than usual?
Case • 43 yo woman with headache x 3 weeks • Presents to hospital with double vision • Low grade fever • On examination, weakness of EOM of left eye, mild proptosis, red eye
What do you see? Sphenoid sinusitis
CT is good at showing… • Bony abnormalities • Acute blood • Large masses (and small enhancing masses if contrast is given) • Calcified intracranial abnormalities • Edema • Large intracranial aneurysms (now we have CTA which is very good at this!!!) • stroke
CT might miss… • Subacute subdural (isodense to brain) • Isodense tumors/infections with little mass effect/edema associated • Small aneurysms • Vasculitis • Vascular malformations • Dural sinus thrombosis • Lesions in the posterior fossa • Demyelination/white matter disease • Stroke • Meningeal processes • Diffuse axonal injury
Yield of CT for headache • CT is generally low yield if a thorough neurologic exam is normal (including LOC/mentation) • CT is higher yield with focal findings, decreased LOC • In typical migraine with normal exam, yield is 0.18%
Normal CT Maxillary sinus air-fluid level Brainstem -medulla
Normal CT Superior ophthalmic vein Sphenoid sinus Temporal lobe Mastoid air cells 4th ventricle Cerebellum
Normal CT Internal carotid artery Basilar artery Pons Temporal horn of right lateral ventricle
Normal CT Left MCA Suprasellar cistern Cerebral aqueduct
Normal CT Cerebral peduncle Interpedulcular cistern
Normal CT Anterior horn of left lateral ventricle Caudate Lentiform Posterior limb of internal capsule Insular ribbon Thalamus Sylvian fissure 3rd ventricle
Normal CT Falx cerebrei Superior sagittal sinus
Raised Intracranial Pressure: What to look for • Loss of basal cisterns • Loss of suprasellar cistern (unilateral or bilateral) • Loss of sulcal/gyral pattern • Loss of grey-white differentiation • Enlarged “trapped ventricles” • Slit-like ventricles
Raised ICP • Do not do an LP if: • you suspect raised ICP • You see a mass or structural lesion with mass effect (e.g. hematoma) • You see mass effect (displaced structures like the falx, uncus, ventricles) • You cannot see the basal cisterns • You see hydrocephalus • You have not done a CT, there are neuro findings/altered LOC and you work in a tertiary care centre where this test is readily available
When should you order CT for headache? • Any unexplained neurologic signs • Altered LOC • New headache type in an older patient • Change in pattern of previous headache • Progressive headache • Thunderclap headache • Refractory headache
Headache Red Flags…CT please! • Abnormal neuro exam • Headache worst on waking in a.m. • Headache waking patient from sleep • Progressive headache • Worse with valsalva • Worse supine than upright • Abrupt onset headache • Other condition predisposing to CNS disease (immune suppressed, cancer, clotting disorder, anticoagulants, recent trauma, etc)
35 yo man, assaulted with pipe Obliteration of ant horn of R lateral ventricle Subarachnoid hemorrhage Epidural hematoma Intracerebral hemorrhage
assault Midline shift
66 yo man with subacute onset of language difficulty Hypodense mass Edema Midline shift
wet Ring enhancing
47 yo man with RA and vertigo Cerebellar hemorrhage
Case • 39 yo man with polycystic kidney disease • CT head was done for headache • Normal neuro exam
What do you see? Small hyperdense lesion
Case • 18 yo girl with a history of ITP • Presents with bizarre behaviour, difficulty walking and headache • On exam appears ‘indifferent’ to her ‘state’ • Moves both sides well with encouragement • Left side ‘lags’ behind when she gets off bed
CT Enlarged cortical veins