Download
1 / 31
310 likes | 1k Views
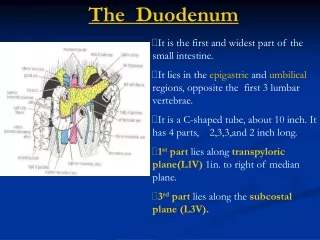
Embryology. Stomach and duodenum develop from the caudal portion of the embryonic foregutDevelopment starts in the 5th week of gestationRate of growth of the left gastric wall >right gastric wall. Anatomy. Cardia

E N D
1. Stomach and duodenumBasic Science Review Donald Baril
October 21, 2004
3. Anatomy Cardia � immediately distal to the GE junction
Fundus � above the GE junction
Body � central portion marked distally by the angularis incisura
Pylorus � distal segment
5. Anatomic relationships Anteriorly: left hemidiaphragm, left lobe of the liver, anterior portion of the right lobe of the liver, parietal surface of the abdominal wall
Posteriorly: left diaphragm, left adrenal, neck, tail, body of the pancreas, aorta and celiac trunk
Inferiorly: transverse colon and its mesentery
6. Blood supply
7. Lymphatic drainage
8. Nervous supply Vagal trunks:
Left � anterior
Hepatic branch
Anterior gastric wall
Right � posterior
Celiac division
Posterior gastric wall
9. Gastric mucosa Lined by simple columnar cells with 3 types of gastric glands:
Cardiac: contain mucus glands, undifferentiated glands and endocrine glands
Oxyntic: contain acid-secreting parietal cells and chief cells that synthesize pepsinogen
Antral: contain gastrin-secreting cells
11. Pepsinogen Synthesized by chief cells
Activated by falling pH level
Catalyzes hydrolysis of peptide bonds
Initiates protein digestion
Most important stimuli for secretion is stimulation of muscarinic receptors
12. Intrinsic factor Secreted by the parietal cells
Necessary for the absorption of vitamin B12 from the terminal ileum
Secretion stimulated by histamine, acetylcholine, and gastrin
Atrophy of the parietal cells, characteristic of pernicious anemia, results in deficiency of IF
13. Acid secretion Basal acid secretion is 2-5 mEq/hr
3 phases:
Cephalic: mediated by cholinergic stimulation
Gastric: stimulated by presence of partially hydrolyzed food and gastric distension
Small peptide fragments and amino acids -> gastrin release
Intestinal: mediated by secretin, somatostatin, peptide YY, and gastric inhibitory peptide
15. Gastric peristalsis Basic electrical rhythm of 3 cycles/minute
Increased contractile activity with the ingestion of food
Pylorus opens and closes every 2-3/seconds, allowing for passage of a small amount of fluid
Remaining fluid is propelled retrograde
16. Peptic ulcer disease 300,000 new cases/year in the U.S.
4 million people receiving medical therapy
Pathogenic factors
Acid secretion: increased basal secretion, increased meal response, abnormal gastric emptying
Environmental: NSAID use, H. pylori infection, cigarette use
Mucosal defense: decreased bicarbonate production, decreased gastric mucosal prostaglandin production
18. Peptic ulcer disease - Pathogenesis Cigarette smoking: alters mucosal blood flow, decreased mucosal PGE2 production and increases acid stimulation
NSAIDs: systemic suppression of PGE2 production
19. Peptic ulcer disease � H. pylori 1886 - ? Relationship between peptic ulcer disease and spiral bacteria
1981 - Robin Warren, M.D., an Australian pathologist, discovered numerous bacteria living in tissue taken during a stomach biopsy.
Spiral urease-producing, Gram-negative bacteria always accompanied changes in the stomach lining
20. Peptic ulcer disease � H. pylori 1982 - Barry Marshall, M.D., joined Dr. Warren in his research
1984 - The Lancet, 100 people undergoing endoscopy, all 13 people with duodenal ulcers and 24 of 28 people with gastric ulcers were infected with Helicobacter pylori
21. Peptic ulcer disease � H. pylori 1984 - Dr. Marshall swallowed a large number of the bacteria himself to test his ideas about H. pylori
For 5 days, he noticed nothing. Then, he began to experience nausea and vomiting
Symptoms resolved on their own after 14 days, an endoscopy on the 8th day revealed that he had developed severe gastritis
22. Peptic ulcer disease � H. pylori 1988 - Marshall and Warren published a report demonstrating the effectiveness of antibiotics in the treatment of peptic ulcers
Randomly assigned 100 people with duodenal ulcers to receive either cimetidine or an antibiotic regimen that targeted H. pylori
Ulcers returned in 90% of people treated with cimetidine
Ulcers returned in only 21% of those whose H. pylori infection was eliminated with an antibiotic and bismuth
24. PUD � Gastric ulcer types Type I � lesser curvature
Antral gastritis and H. pylori infection often present
Type II � prepyloric
Occur in association with duodenal ulcers
Type III � antrum
Result from NSAID use
Type IV � lesser curvature, near the GE junction
Similar pathophysiology to type I
25. PUD � Clinical features Patients present with epigastric pain
Typically worse in the morning
Burning, stabbing, gnawing
Commonly relieved by eating or taking antacids
Patients may present acutely with bleeding, perforation, or obstruction
26. PUD - Diagnosis Barium contrast study or endoscopy
27. PUD � H. pylori and diagnosis Serology � reliable marker of initial infection
Remains + even after the eradication of bacteria
Urea breath test � more reliable marker of active infection
Labeled urea is converted into ammonia and labeled carbon dioxide by the H. pylori urease in the stomach
Endoscopic biopsy
28. PUD � Medical Treatment
30. Surgical treatment of PUD Indicated for failures of medical treatment and in patients presenting with complications
Truncal vagotomy with drainage (pyloroplasty, antrectomy, or gastrojejunostomy)
Proximal gastric vagotomy
Highly selective vagotomy
31. HSV
<1% operative mortality
1% risk of persistent dumping sxs
10-15% risk of recurrent ulceration TV and drainage
1-2% operative mortality
TV/antrectomy
1-2% risk of recurrent ulceration
10-15% risk of persistent dumping sxs
TV/pyloroplasty
10% risk of recurrent ulceration
1% risk of persistent dumping sxs
32. Physiological changes after truncal vagotomy Gastric effects
Decreased basal acid output
Decreased maximal acid output
Increased fasting and postprandial gastrin
Gastrin cell hyperplasia
Accelerated liquid emptying
Nongastric effects
Decreased pancreatic exocrine secretion
Decreased postprandial bile flow
Diminished release of vagally mediated peptide hormones
33. Gastric surgery complications - Dumping syndrome Delivery of hyperosmotic fluid to the small bowel leading to massive fluid shifts
Sxs: postprandial palpitations, sweating, weakness, dyspnea, nausea, cramps, diarrhea, syncope
Dx: hyperosmolar glucose load will elicit sxs
Tx: multiple small, low-fat, low-carbohydrate meals that are high in protein
Preprandial octreotide may reduce sxs
34. Gastric surgery complications - Alkaline reflux gastritis Reflux of bile into stomach following BI, BII, or pyloroplasty
Sxs: Postprandial pain, bilious emesis
Dx: Endoscopy, HIDA scan
Tx: Cholestyramine, reglan, acid-suppression
Surgical tx: conversion to Rou-en-Y gastrojejunostomy
35. Gastric surgery complications
36. Perforated peptic ulcer Incidence of perforation is 5-10% of all patients with peptic ulcer disease
Incidence of perforation has not decreased proportional to the overall decline in peptic ulcer disease over the past few decades
Perforation is often the first clinical presentation of the disease
37. Perforated peptic ulcer Mortality of 1-20%
Accounts for 70% of deaths associated with PUD
Negative prognostic factors include presence of comorbid conditions, > 24 hours since time of perforation to time of repair, presence of shock
38. Perforated peptic ulcer - Presentation Sudden onset of severe upper abdominal pain
May be referred to back or shoulder
Boardlike rigidity
Mild leukocytosis
Mildly elevated serum amylase levels
Dx based on upright CXR in 85% of cases
Most commonly occurs on anterior gastric or duodenal wall
39. Perforated peptic ulcer � Treatment options Simple closure
Simple closure with overlying omental patch
Simple closure with fibrin glue sealing
Closure with Graham patch
Simple closure with overlying omental patch or Graham patch closure with:
truncal vagotomy
proximal gastric vagotomy
highly selective vagotomy
40. Timing of acid reduction Patients are selected for an immediate acid-reducing procedure after perforation if:
Perforation less than 24 hours
No comorbid conditions
No evidence of shock
History of sxs > 3 months
In these patients, ulcer recurrence is < 10% with no additional perioperative morbidity or mortality
41. Timing of acid reduction If the traditional criteria are met, acid-reduction surgery is strongly indicated in patients who:
have previously failed an H. pylori eradication regimen
are known to be not infected by H. pylori
have suffered other complications of PUD (including bleeding and/or obstruction)
are NSAID dependent
42. Gastric cancer Incidence in U.S. 10/100,000
Incidence in Japan 78/100,000
10th most common cancer
5-year survival in U.S. is 12%
5-year survival in Japan in 53%
Overall incidence in U.S. is decreasing
43. Gastric cancer � Risk factors Environmental/general: dietary nitrites, smoking, H. pylori infection, black race, male gender, low socioeconomic class
Gastric: chronic atrophic gastritis, hypochlorhydric or achlorhydric state, pernicious anemia, adenomatous polyp, previous gastric surgery
44. Pathology of gastric cancer 95% of gastric cancers are adenocarcinomas
Remaining 5% includes lymphoma, carcinoid, GISTs, and squamous cell
Macroscopically divided into ulcerative (75%), polypoid (10%), scirrhous (10%), and superficial (5%)
Histologically divided into intestinal and diffuse
Over past few decades, increase in proximally occurring tumors
45. Presentation of gastric cancer Vague epigastric discomfort
Anorexia
Weight loss
Vomiting
Dysphagia
Palpable mass in up to 30% of patients
10% present with evidence of metastatic disease (Virchow�s node, Sister Mary Joseph�s node, Blumer�s shelf, ascites, jaundice)
46. Surgical treatment of gastric cancer Total gastrectomy with Roux-en-Y reconstruction
Advocated for proximal and midbody tumors
Subtotal gastrectomy
Advocated for distal tumors
Entails resection of � of the stomach
5-6 cm resection margin when possible
? Splenectomy
Routine splenectomy does not improve survival but does increase morbidity and mortality
48. Lymphadenectomy in gastric cancer Role of extended lymphadenectomy in gastric cancer remains controversial
Current recommendation is D1 dissection
D1: removal of all nodal tissue within 3 cm of the primary tumor
D2: D1 + clearance of hepatic, splenic, celiac, and left gastric lymph nodes
D3: D2 + omentectomy, splenectomy, distal pancreatectomy, and clearance of porta hepatis lymph nodes
49. Gastric lymphoma Increasing in incidence
Accounts for 2/3 of GI lymphoma
Average age at presentation is 60
Endoscopy permits diagnosis in 90% of patients
Most lesions are located in the distal stomach, spread locally by submucosal infiltration
Initial treatment is chemotherapy: doxorubicin and cyclophosphamide
Surgery reserved for patients with an incomplete response or a recurrence
50. Gastroduodenal Crohn�s Prevalence of 0.5-13% in patients with ileocolonic disease
UGI involvement is typically in the antrum and duodenal bulb
Sxs include epigastric pain and dyspepsia
Hematemesis and melena are rare
51. Gastroduodenal Crohn�s Duodenal fistula are rare (0.5%)
Fistulae involving the stomach almost always originate from the colon or small bowel
Corticosteroids are the mainstay of medical tx
Unknown role of acid reduction therapy
52. Surgery for gastroduodenal Crohn�s Gastrojejunostomy
Most commonly performed surgery for gastroduodenal Crohn�s
Indicated for obstruction and fistulization
Unknown role for vagotomy
Stricturoplasty
?Advantageous compared to gastrojejunostomy given less mobilization of small bowel
53. Which of the following statements is/are true regarding the arterial supply to the stomach: A) The right gastric artery, a branch of the SMA supplies the gastric antrum
B) Gastric viability may be preserved after ligation of all but one major artery
C) In cases of celiac artery occlusion, gastric viability is maintained collaterally through pancreaticoduodenal arcades
D) The left gastroepiploic artery is a branch of the celiac trunk
54. At a cellular level, the major stimulant(s) of acid secretion by the gastric parietal cell is/are: A) Histamine
B) Prostaglandin E2
C) Acetylcholine
D) Gastrin
E) Norepinephrine
55. Which of the following statements is/are correct regarding intrinsic factor: A) Intrinsic factor is produced in chief cells located in the gastric fundus
B) Total gastrectomy is following by folate deficiency caused by vitamin malabsorption due to intrinsic factor deficiency
C) Secretion of intrinsic factor, like that of acid, is stimulated by gastrin, histamine, and acetylcholine
D) Intrinsic factor deficiency accompanies antral gastritis caused by H. pylori infection
56. Gastrin release is increased by which of the following: A) Antral acidification
B) Ischemia
C) Histamine
D) Antral distension
E) Trauma
57. Appropriate treatment for a perforated ulcer in a 35-year old male who has been treated for peptic ulcer disease for the past 7 years and is hemodynamically stable is: A) Nasogastric suction and antibiotics
B) Closure of the perforation
C) Parietal cell vagotomy and pyloroplasty
D) Truncal vagotomy and gastroenterostomy
58. Which of the following statements is/are correct with regard to pyloric obstruction secondary to peptic ulceration: A) Pyloric obstruction is suggested by hypochloremic hyponatremic alkalosis
B) Pyloric obstruction is suggested by hypochloremic hypokalemic alkalosis
C) Approximately 80% of patients with benign gastric outlet obstruction obtain permanent relief with endoscopic balloon dilatation
D) The lifetime risk of pyloric obstruction among patients with peptic ulcer is 40%
59. 50 yo M underwent truncal vagotomy with BII reconstruction 2 yrs ago. He now has postprandial pain, nausea, bilious emesis. Endoscopy reveals bile in the stomach evidence of severe gastritis. Appropriate therapy would include: A) Octreotide administration
B) Conversion of BII gastrojejunostomy to BI gastroduondenostomy
C) Conversion of BII gastrojejunostomy to Roux-en-Y gastrojejnostomy
D) Roux-en-Y hepaticojejunostomy
60. Which of the following conditions is considered to increase the risk of gastric cancer: A) Pernicious anemia
B) Previous partial gastrectomy
C) Gastric hyperplastic polyps
D) Gastric adenomatous polyps
61. With regard to operative management of gastric carcinoma, which of the following is/are correct: A) Resection margins of 2 cm are necessary to prevent recurrence due to intramural metastasis
B) Prophylactic splenectomy has been shown to improve outcome among similarly staged patients
C) Extended lymphadenectomy that includes nodes along the aorta and esophagus has not been shown to improve survival in North American trials
D) Long-term survival is rare if adjacent organs must be resected to achieve local control
62. Which of the following statements regarding gastric lymphoma is/are correct: A) More than one-half of GI lymphomas occur in the stomach
B) The peak incidence of gastric lymphoma is in the 2nd and 3rd decades of life
C) Endoscopic biopsy provides enough information for a diagnosis in 90% of cases
D) Gastric perforation occurs among 40% of patients treated with cytolytic agents instead of gastrectomy