Download

1 / 27
300 likes | 888 Views
Myasthenia Gravis 重症肌无力(MG). Department of Neurology Ruijin Hospital. 1. Outline . Introduction Etiology and Pathogenesis Pathology & Pathophysiology menifestation Diagnosis& Differential Diagnosis Management. 2. Introduction. Acquired autoimmune disease

E N D
Myasthenia Gravis重症肌无力(MG) Department of Neurology Ruijin Hospital 1
Outline Introduction Etiology and Pathogenesis Pathology&Pathophysiology menifestation Diagnosis&Differential Diagnosis Management 2
Introduction Acquired autoimmune disease Inability of signal transmission within the neuro-muscular junction (NMJ) Clinically characterized by: Fatigue of skeletal muscles Deterioration on movement Alleviation on cholinesterase inhibitors Incidence: (0.5-5)/100,000 Prevalence: 10/100,000 3
Etiology and Pathogenesis Normally when impulses travel down the nerve, the nerve dendings resealse a neurotransmitter substance called acetylcholine, Ach tracels through the neuromuscular junction and binds to Ach receptors which are activited and generate a muscle constration. The chronic inflammation of MG causes several changes in the structure of the Neuromuscular Junction which also inhibit transmission and contribute to weakness. These include flattening out of the junctional folds, spreading out of AChR and Acetylcholinesterase, a 66% decrease in number of AChR, and an increased junctional gap.
Pathology Muscular morphology was normal in most cases loss of synaptic folds and widened clefts thymoma with MG • Hypertrophy(65%) • Thymoma(10-20%) muscles contain lymphorrhages 5
Clinical Presentation-(1) MG occurs at any age Onset summit: 20-40y(F>M), 40-60y(M>F) 10% onset before 10y Thymoma was frequently seen in late onset patients Mostly insidious and progressive Muscle weakness
Clinical Presentation-(3) Weakness could be seen in all skeletal muscles. Ptosis,diplopia,oropharyngealmuscle weakness –difficulty in swallowing and talking, or limb weakness fluctuatesand progressively worsens over course of day worsens with prolonged use of affected muscles (i.e.fatiguable)
Ocular Ptosis(dropping eyelid) – asymmetric, fatigues with upgaze Diplopia(double vision) – most common involved MR(medial rectus ) 9
Bulbar Respiratory muscles • Dysarthria • Dysphagia • Dysphonia • Masticatory weakness • – jaw closure > jaw open • Exertional dyspnea • Tachypnea • Respiratory failure (Myasthenic crisis) Axial muscles Limbs • Neck flexion • Neck extension • Commonly proximal, symmetric • Arms more affected than legs 10
MG Crisis defined as the need for assisted ventilation arises in about 10% of myasthenic patients more likely to occur in patients with dysarthria, dysphagia, and documented respiratory muscle weakness may also occur in other patients after respiratory infection or major surgery Clinical Presentation-(5) 11
Categorization of MG Crisis Myasthenic crisis acetylcholine insufficiency Cholinergic crisis acetylcholine overmuch Brittle crisis non susceptivity to acetylcholine Clinical Presentation-(5) 12
Osserman Classification of MG-(1) Based on the severity of the disease 1、Adult MG Ⅰ.Ocular myasthenia(15-20%) Ⅱ(a).Generalized MG of mild intensity(30%) Ⅱ(b) .Generalized MG of moderate intensity(25%) Ⅲ.Severe generalized disease(15%) with respiratory failure: Intubation needed to maintain airway Ⅳ. generalized disease due to type Ⅰ,Ⅱ(a),Ⅱ(b) getting worse Ⅴ.Myasthenic Gravis with muscle atrophy in early stage. 14
Osserman Classification of MG-(2) 2、Childhood MG (account for 20% in Chinese MG patients) (1) Neonatal MG: most cases recovered after 1w to 3ms’ treatment (2) Congenital MG: mostly resistant to AchR inhibitors; family history 3、Teenager MG: onset from 14y to 18y. Most cases only presented with ocular symptoms 15
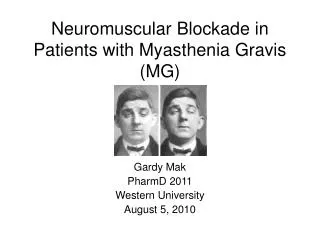
Diagnostic tests • Fatigue test(Jolly test) • Blink eyes for 30 consecutive times • Holding arms horizontally • Crouching for 10-20 consecutive times • Neostigmine Test • 1.5mg neostigmine methylsulfate for adults • Alleviation within 10-20m post injection is (+) • 0.5mg atropine was simultaneously injected for prevention of side effects
Neostigmine test A: Severe ptosis of the lids. B: Same patient 1 minute after intravenous injection of edrophonium (10 mg). (From Rowland LP, Hoefer PFR, Aranow H Jr. Myasthenic syndromes. Res Publ Assoc Res Nerv Ment Dis 1961;38; with permission.) 17
Repetitive nerve stimulation Single fiber electromyography Diagnostic tests 18
Diagnostic tests 1.Antibodies to AChR generalized MG :>80% iocular MG:50% MG and thymoma:98-100% The titer does not match the severity of symptoms 2. Anti-muscle specific receptor tyrosine kinase (MuSK) antibodies Used if MG suspected, patient seronegative Present in 40–50% of seronegative patients with generalized MG; absent in ocular MG 19
Radiographs of the chest provide evidence of thymoma in about 15% of patients, especially in those older than 40 years. CT of the mediastinum demonstrates all but microscopic thymomas. Diagnostic tests-(5) thymoma hyperplasia of the thymus 20
Diagnosis Procedure When to suspect? Fluctuating Weakness Better in the morning, worse in the afternoon Positive fatigue test How to confirm? Neostigmine test Repetitive nerve stimulation SFEMG Anti-AchR antibody titters 21
Differential diagnosis Lambert-Eaton syndrome Chronic inflammatory muscular disorders Ocular muscle dystrophy Progressive bulbar palsy Clostridium botulinum intoxication 22
Management-(1) Management with medicine Anticholinesterase drug(Mestinon max60mg,q4h) Cortisones(could worsen the disease in short term, side effects could be fatal) Immune suppress agents(azathioprine, cyclophosphamide, cyclosporine A, etc) Contraindicated drugs 23
Management-(2) Thymus-targeted therapy indication thymoma, hypertrophy of thymus, drug-resistant patients contra-indication <18y, non-severe effective for 70% patients sometimes worsens 24
Management-(3) Plasmapheresis remove Ach-R antibodies of serum effective but not consistent used in case of MG crisis Intravenous Immunoglobulin (IVIg) effective side effects were rare widely used in clinical practice 0.4g/(kg d), iv. 3-5 days/course interfere the function of Ach-R antibodies 25
Artificially facilitated breath is urgently needed Anti-infection therapy is frequently needed Cortisones Myasthenia Crisis: increase doses of neostigmine Choligernic Crisis: stop using neostigmine Brittle Crisis: stop using neostigmine Management-(4) 26
Summary Acquired autoimmune Disease Antibodies attack the Acetylcholine receptor. the ocular, bulbar and proximal skeletal are more likely affected Fatigability is a key symptom! Disease has a fluctuating pattern of ‘crises’ and remittances. Treatment is usually with Acetylcholinesterase inhibitors and immunosupression Easily treated and would have a good life expectancy. 27
Thanks! 28