Download
1 / 49
550 likes | 1.08k Views
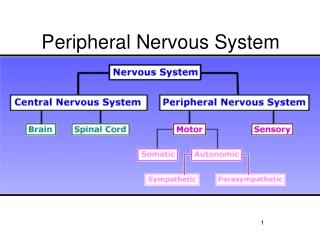
Nursing Care of Patients with Peripheral Nervous System Disorders . Rita Carey-Nita . Neuromuscular Disorders . Neuromuscular Disorders involve a disruption of the transmission of impulses between neurons and the muscles they innervate They include: Multiple Sclerosis Myasthenia Gravis

E N D
Nursing Care of Patients with Peripheral Nervous System Disorders Rita Carey-Nita
Neuromuscular Disorders Neuromuscular Disorders involve a disruption of the transmission of impulses between neurons and the muscles they innervate They include: • Multiple Sclerosis • Myasthenia Gravis • Amyotrophic Lateral Sclerosis
Multiple Sclerosis Pathophysiology • MS is a chronic progressive degenerative disease that affects the myelin sheath of the neurons in the CNS • The myelin sheath begins to break down as a result of the activation of the immune system • The nerve becomes inflamed and edematous • Nerve impulse slows • With progression of disease scarring or sclerosis of nerve occurs • Nerve impulse become blocked causing permanent muscle function loss
Etiology • Unknown May be: • Autoimmune process • May be result of viral infection • Hereditary • Environmental triggers Onset is usually between 20-50 years old Women twice as often than men May be mild or may be permanently debilitating
Etiology Symptoms may begin slowly over long period of time or suddenly & progressive faster Characterized by remissions and exacerbations Triggers • Extreme heat or cold • Fatigue • Infection • Physical or emotional stress • Hormonal changes as in pregnancy
Signs & Symptoms • Muscle weakness/paralysis of limbs, trunk or dead • Ataxia • Results in falls & accidents • Tingling sensation • Numbness • forgetfulness/difficulty concentrating • Visual disturbances • One eye at a time • May have pain on eye movement • Diplopia • Blurred vision • Patchy blindness
Signs & Symptoms • Fatigue • Muscle spasticity • Bowel or bladder dysfunction • Dysarthria • Dizziness/vertigo • Impaired hearing • Tinnitus • Constipation • Spastic bladder • Sexual dysfunction • Anger—depression—euphoria
Diagnostic Tests • History and Physical • Signs & Symptoms • CSF fluid may show increase in oligoclonalimmunoglobin G • MRI shows sclerotic plaques
Therapeutic Interventions • No cure • Interferon treatment reduces exacerbations • Betaseron—Avonex • Steroids decrease inflammation and edema of neuron • Adrenocorticotropic—prednisone—corticotropics • Immunosuppresant depress immune response • Imuran—Cytoxan • Anticonvulsants decrease neuropathic pain • Dilantin—Tegretol • Parasympathetic agents help with bladder issues • Urecholine—Ditropan • Muscle spasm may be controlled with • Valium—Liorseal—Zanaflex • Fatigue is treated with antidepressants or Symmetrel (antiviral)
Therapeutic Interventions • Rehabilitation • PT • OT • ST • Plasmaphersis • Removes plasma portion of whole blood and replaces it with fresh plasma • Removes antibodies that may be attacking the myelin sheath • Hope is to suppress the immune response and inflammtion
Nursing Interventions • Teach to avoid triggers that can cause exacerbation • Rest—exercise—stress reduction or avoidance—balanced diet • Monitor airway due to muscle weakness • Resp rate—depth—oxygen saturation—cough & deep breathe—suction • Monitor for dysphagia • HOB elevated—monitor cough & gag reflex—ST—swallowing precautions—soft diet—thickened liquids • Mobility • AROM & PROM—PT—OT—reposition frequently if immobile
Myasthenia Gravis • Myasthenia Gravis is weakness of the voluntary muscles of the body • Disease of the neuromuscular junction • The neuron release the neurotransmitter acetycholine across the synaptic cleft which cause muscle contraction • With MG antibodies attack and destroy acetycholine receptors sites at the neuromuscular junction • Result is inability to stimulate muscle contraction and therefore loss of voluntary muscle strength
Signs & Symptoms • Progressive extreme weakness • Hallmark sign—increase weakness with activity with improved strength with rest • Affects eye and eyelid movement • Ptosis • Chewing • Swallowing • Breathing • Masklike expression • Voice fades with long conversation
Exacerbations & Remissions • Triggers • Emotional & physical stress • Pregnancy • Illness • Trauma • Extreme temperatures • Surgery • Medications that block action at neuromuscular junction • Electrolyte imbalance
Complications • Aspiration • Respiratory infection • Respiratory failure • Mysathnic crisis • Not enough medication • Results in • Ptosis—dysphagia—dysarthria—dyspnea—weakness • Cholinergic crisis • Overmedication with anticholinesterase • Results in • Increased muscle weakness—dyspnea—nausea & vomiting—salivation—abd cramping—sweating—increased bronchial secretions—miosis
Diagnostic Test • Diagnosis based on history & physical • Patient looks up for 2-3 minutes—ptosis will occur with MG • With rest eyelids open without difficulty • IV Tensilon given—if muscle strength improves dramatically MG diagnosed • EMG to rule out other causes of symptoms • PFT’s to determine to predict myasthenic crisis leading to respiratory failure
Therapeutic Intervention • No Cure • Treatment aimed at control symptoms • Thymectomy to decrease the production of Ach receptor antibodies and decrease symptoms • Anticholinesterase drugs destroys acetycholinesterase that breaks down ACh allowing for ACh to attach to muscles causing contraction therefore strength increases • Prostigmin—Mestinon • Steroids suppress immune response • Prednisone—Prednisolone • Plasmapheresis to remove antibodies from plasma
Nursing Care • Monitor & teach patient signs of • Myasthenic crisis • Cholinergic crisis • Schedule anticholinesterase medication to peak during times of most activity • Teach • patient importance of well balance diet • How to conserve energy with daily activities • Avoidance of persons with infections • Teach patient to avoid medications that will exacerbate weakness • Beta-blockers—calcium channel blockers—quinine—quinidine—procainamide—D penicillamine—alpha-interferon—botulinum toxin—neuromuscular blocking agents
Amyotrophic Lateral Sclerosis ALS also called Lou Gehrig’s disease • Progressive degenerative neuromuscular condition • Affects motor neurons responsible for voluntary muscles • Upper and lower motor neurons begin to degenerate and form scar tissue or die blocking nerve impulses from brain and spinal cord • Muscle tissue atrophy occurs decreasing muscle strength and coordination • With progression more muscle groups are affected • Unable to breathe and swallow • Cognitive function remains unaffected
Etiology • Occurs at any age • No known cause • Genetic tendency in some cases • Onset between 40-70 years • More often in men than women
Signs & Symptoms • Progressive muscle weakness leads to complete immobility • Decreased coordination of arms—legs—trunk • Atrophy of muscles • Fasciculations • Muscle spasms that cause pain • Difficulty chewing & dysphagia lead to aspiration • Inappropriate emotional outbursts • Dysarthria—progresses to complete inability to speak • Constipation • Urinary urgency—hesitancy—frequency
Complications • Malnutrition • Falls • PE • CHF • Death related to respiratory complications • Atelectasis—pneumonia—respiratory failure—ventilator dependence • Death occurs within 3-5 years of diagnosis usually due to respiratory failure • Only 10% live 10 years or more
Diagnostic Tests • CSF analysis • EEG • EMG • Blood enzymes increase with muscle atrophy
Therapeutic Interventions • Maintain function • Emotional support to patient & family • Baclofen—Diazepam for muscle spasms • Quinine for muscle cramps • Riluzole to reduce damage to motor neurons & prolong life • PT—OT • ST • AAC such as laptop computer • Massage • Position change & skin care • Enteral feedings • Prevention of infection • Support Groups • Counseling
Guillain-Barre Syndrome GBS is also called acute inflammatory polyneuropathy • Inflammatory disorder characterized by abrupt onset of symmetrical paresis that progress to paralysis • Destruction of myelin sheath of spinal and cranial nerves occurs due to the diffuse inflammatory reaction • Peripheral nerves are infiltrated with lymphocytes leading to edema and inflammation • Segmental demyelination cause axonal atrophy slowing or blocking nerve conduction • Begins distal and ascends manner • Remyelination slowly occurs in a descending manner with resolution of symptoms
Guillain-Barre Syndrome • Ascending GBS • Progressive weakness and numbness beginning in legs and ascending up the body • Numbness mild but muscle weakness leads to paralysis • Ascends all the way to cranial nerves • Deep tendon reflexes depressed or absent • Respiratory function impaired 50% of time • Descending GBS • Less common • Affects cranial nerves that originate in brain stem • Dysarthria • Dysphagia • Respiratory function impairment rapid • Numbness more in hands than feet • Diminshed or absent reflexes
Guillain-Barre Syndrome • Miller Fisher syndrome • Rare • No respiratory compromise or sensory loss • Profound ataxia • Absence of reflexes • Paralysis of extraocular muscles • Pure motor GBS • Milder form • Mimics ascending GBS • Does not have numbness or paresthesias
Etiology • Exact cause unknown • Possible autoimmune response to viral infection or vaccination • Viral illness noted within 2 weeks prior to onset of symptoms • Usually occurs between 20-50 years old • 45 or older more often • Affects men and women equally • 50% higher incidence in Caucasians than African Americans
Signs & Symptoms Three stages • Stage One • Start with onset of symptoms and lasts until progression stops • 24 hours to 3 weeks • Abrupt onset of muscle weakness and paralysis • Little or no muscle atrophy • Recent history of viral illness or vaccination • Extent of respiratory impairment is dependent on type of GBS • May require intubation and mechanical ventilation • Labile blood pressure—cardiac dysrhythmias—urinary retention—paralytic ileus—numbness—cramping—pain
Guillain-Barre Syndrome • Stage two • Symptoms most severe but progression has stopped • 2-14 days • Stage three • Recovery stage • Axonal regeneration and remyelination occurs • 6 – 24 months • Symptoms improve slowly • Takes months to a year to recover • Few patients suffer chronic disability
Complications • Respiratory Failure • Infection • Depression • Pneumonia • UTI • Complications of immobility • PE—DVT—Impaired skin intergrity—muscle atrophy
Diagnostic Tests • Lumbar puncture to obtain CSF • Elevated protein • EMG • Nerve Conduction Velocity tests • PFT’s
Therapeutic Interventions First stage • Complete care • Oxygen & mechanical ventilation • Plasmapheresis within 7-14 days of onset Second phase—plateau phase • Emotional support Third phase—recovery phase • Intensive rehabilitation
Nursing Care Supportive • Monitor respiratory function • Monitor swallowing • Pain management • Enteral feedings • Communication board • Diversional activity during recovery phase
Patient Education • Explain all procedures • Disease process—sign & symptoms—recovery • Discuss need for intubation as respiratory function may be impaired
Postpolio Syndrome Postpolio Syndrome • Condition that affects survivors of polio 10-40 years after recovering from infection of poliomyelitis virus • Severity depends on degree of residual weakness and disability from initial illness
Signs & Symptoms • Further weakness of muscles that were affected initially with polio virus • Fatigue to progressive weakness to atrophy • Sleeping difficulties • Joint pain • Scoliosis • Respiratory compromise Symptoms vary from mild to debilitating
Postpolio Syndrome Diagnostic Tests • History and Physical Exam Therapeutic Interventions • None other than rest and moderate exercise
Review Table 50.4 Summary of PNS Disorders • Review Box 50.3 Nursing Care Plan for Patients with Progressive Neuromuscular Disorder
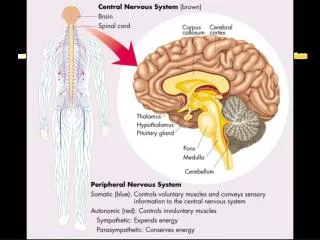
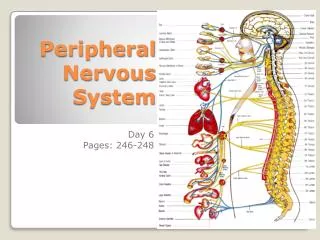
Cranial Nerve Disorders • There are 12 pairs of cranial nerves that originate in the brain • They innervate the head—neck—special sensory organs • Cranial nerve disorders are classified as peripheral neuropathies • Disorders affect sensory—motor—or both of a single nerve • Cause can be unknown or may include: • Tumors—infection—inflammation—trauma • Two common cranial nerve disorders are • Trigeminal neuralgia • Bell’s palsy
Trigeminal Neuralgia Trigeminal Neuralgia is also called tic douloureux • Affects 5th cranial nerve—trigeminal nerve • Has 3 branches that have both sensory & motor function • Innervates the forehead—nose—cheek—gums—jaw • TN only affects the sensory portion of nerve • Irritation or chronic compression of nerve initiates symptoms • Seen more often in women between 50-60 years old
Trigeminal Neuralgia Signs & Symptoms • Intense recurring pain in the skin of one side of the face • Sudden jabbing, burning, knifelike pain • Onset begins & ends suddenly lasting a few seconds to minutes • Occurs in clusters that can be many times or few • Slight touch—cold breeze—talking—chewing are triggers • Trigger zones include: • Lips—upper & lower gums—cheeks—forehead—side of nose • Sleep provides relief • Frequent blinking and tearing of eye on affected side
Trigeminal Neuralgia Therapeutic Intervention • Anticonvulsants reduce nerve impulses • Dilantin—Tegretol • Baclofen—clonazepam—gabapentin—valproic acid • Help control symptoms • May cause bone marrow suppression so need routine CBC • Nerve block with local anesthetic • 6-8 months relief • Surgery if all else fails • Radio frequency ablation to destroy some nerve branches • Results are anesthesia of area • Gamma Knife radiosurgery • Creates lesion on nerve which blocks pain signal
Trigeminal Neuralgia Patient Education • Eye (cornea) on affected side needs to be protected from injury due to loss of sensation • Goggles—sunglasses—eye patch at night • Artificial tears
Bell’s Palsy Pathophysiology • Affects cranial nerve VII—facial nerve • Inflammation and edema of nerve causes interruption of nerve impulse • Loss of motor control on one side results • Contracture of facial muscle can occur if slow recovery Etiology • Nerve trauma by viral or bacterial infection • May be autoimmune • Affects men and women equally • Affects all ages • Any time of year • More common in: • 3rd trimester of pregnancy—immunocompromised—diabetics
Bell’s Palsy Signs & Symptoms • Onset abrupt & progresses over 2-5 days • Pain behind ear may precede onset of facial paralysis • Dry eye • Tingling around lips • Inability to close eyelid—wrinkle forehead—smile—close lip • Mouth pulled to unaffected side • Drooling on affected side • Constant tearing of affected eye • Loss of taste on anterior 2/3 of tongue • Dysarthria • Severity of paralysis peaks within several days of onset
Bell’s Palsy Diagnostic Tests • 50 % of patients recover completely in short time • 35% within one year • History & Physical • Need to rule out CVA Therapeutic Interventions • Prevention of complications • Protect cornea eye on affected side • Prednisone for 7-10 days to decrease edema • Antiviral medication • Moist heat • Gentle massage • Facial sling
Review the Nursing Diagnosis on 1140 • Review table 50.5 to summarize Cranial Nerve Disorders