Download
1 / 26
410 likes | 729 Views
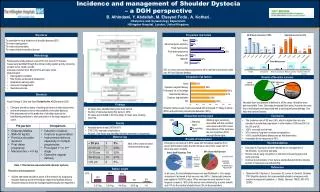
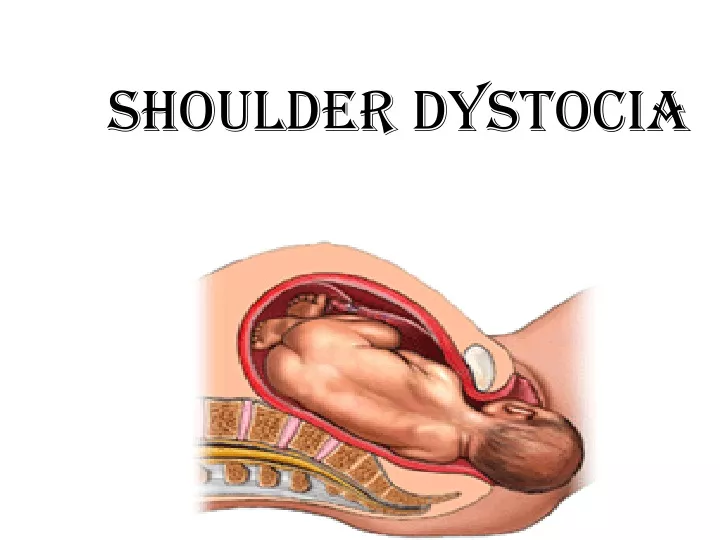
Shoulder Dystocia. Definition and Diagnosis. Difficulty encountered in the delivery of the fetal shoulders after delivery of the head. Due to impaction of the fetal shoulder behind the symphysis pubis. PATHOPHYSIOLOGY.

E N D
Definition and Diagnosis • Difficulty encountered in the delivery of the fetal shoulders after delivery of the head. • Due to impaction of the fetal shoulder behind the symphysis pubis.
PATHOPHYSIOLOGY • The fetal bisacromial diameter normally enters the pelvis at an oblique angle with the posterior shoulder ahead of the anterior one, rotating to the anterior-posterior position at the pelvic outlet with external rotation of the fetal head.
Risk Factors • Maternal • Antenatal Factors • Abnormal pelvic anatomy • Gestational diabetes • Post-dated pregnancy • Previous shoulder dystocia • Short stature
Intrapartum Factors • Prolonged Second Stage of Labor • Oxytocin Induction • Midforceps and Vacuum Extraction 2. Fetal • Suspected macrosomia • Male sex
Diagnosis • head recoils against perineum, ‘turtle’ sign • spontaneous restitution does not occur • failure to deliver with expulsive effort and usual gentle direction
Fetal Complications • Fetal Fractures - • In 18 to 25% of cases • Erb’s Palsy - • Although 80% will resolve by 18 months • Perinatal Asphyxia - Uncommon • Neonatal Death - Rare
Maternal Complications • Vaginal Lacerations • Cervical Lacerations • Postpartum Hemorrhage • Puerperal Infection
Management • Know the Drill! CALL FOR HELP REMAIN CALM CALL FOR HELP REMAIN CALM Oh, and by the way, don’t forget to call for help.
Seek Help from • Individuals who MUST be present : • Attending physician • Anesthesiologist • Pediatrician • Nursing Staff • “Extra Hands”
Management Ask for help Lift - the buttocks and legs Anterior disimpaction of shoulder- rotate to oblique and give suprapubic pressure Rotation of the posterior shoulder - Woods’ manoeuver Manual removal of posterior arm
Avoid the P’s • Panic • Pulling (on the head) • Pushing (on the fundus) • Pivoting (head)
It is important that the conduct of any shoulder dystocia be managed by the most experienced person in the room. • This individual ( generally the attending physician) must have the ability to intervene at any time and should be the only one giving orders.
The Principle Maneuvers • Gentle Traction (?) • McRoberts Maneuver • Suprapubic Pressure • Woods’ Corkscrew Maneuver • Delivery of the Posterior Arm
Preliminary Measures: • Gentle pressure on the fetal vertex in a dorsal direction will move the posterior fetal shoulder deeper into the maternal pelvic hollow, usually resulting in easy delivery of the anterior shoulder.
McRobert’s Maneuver • Marked flexion of the maternal thighs unto the abdomen • Decreases the angle of pelvic inclination • Cephalic rotation of the pelvis frees the anterior shoulder
Suprapubic Pressure • Moderate suprapubic pressure is often the only additional maneuver necessary to disimpact the anterior fetal shoulder. Stronger pressure canonly be exerted by an assistant.
Woods’ Corkscrew Maneuver • The shoulders must be rotated utilizing pressure on the scapula and clavicle. • The head is never rotated.
Woods’ Corkscrew Maneuver • Del may be facilitated by counterclockwiserotation of the ant shoulder to the morefavorable oblique pelvic diameter, or clockwise rotation of the posterior shoulder. • During these maneuvers, expulsive efforts should be stopped and the head is never grasped !!
Delivery of the Posterior Arm • To bring the fetal wrist within reach, exert pressure with the index finger at the antecubital junction.
Delivery of the Posterior Arm • Sweep the fetal forearm down over the front of the chest.
Delivery of the Posterior Arm • manipulative delivery of the posterior arm by inserting a hand into the posterior vagina and ventrally rotating the arm at the shoulder with delivery over the perineum.
When All Else Fails... • Cleidotomy • The Zavanelli Maneuver • Symphysiotomy
The Zavanelli Maneuver • First described in 1988 • Consists of cephalic replacement and then cesarean delivery.