Download
1 / 19
220 likes | 718 Views
Shoulder Dystocia Review July 24, 2014. Marie-Claude Laplante Paula Tchen MS3. Objectives. 10553 Propose & execute immediate management of shoulder Dystocia. 10554 Describe options if immediate management of shoulder Dystocia is not successful. Definition.

E N D
Shoulder Dystocia ReviewJuly 24, 2014 Marie-Claude Laplante Paula Tchen MS3
Objectives • 10553 Propose & execute immediate management of shoulder Dystocia. • 10554 Describe options if immediate management of shoulder Dystociais not successful.
Definition • Abnormal labour or dystocia (means difficult labour or childbirth) • Occasionally referred to as failure to progress. • A vaginal delivery is complicated by shoulder dystocia when, after delivery of the fetal head, additional obstetric maneuvers beyond gentle traction are needed to enable delivery of the fetal shoulders. • *leading indication for primary C/S in the US • variability in the diagnosis, management and criteria for dystocia • Rarely diagnosed with certainty
Pathophysiology of shoulder dystocia • During delivery the anterior shoulder should slide under the symphysispubis. If the fetal shoulders remain in an anterior-posterior position during descent or descend simultaneously rather than sequentially into the pelvic inlet, then the anterior shoulder can become impacted behind the symphysis pubis; the posterior shoulder may be obstructed by the sacral promontory. Anterior obstruction is more common than posterior obstruction. If descent of the fetal head continues while the anterior or posterior shoulder remains impacted, then stretching of the nerves in the brachial plexus may occur and may result in nerve injury. • If fetal head is turned to one side (asynclitism) or extended (extension) the cephalic diameter is increased. Brow presentation can cause dystocia if it does not convert to vertex or face.
Epidemiology of shoulder dystocia • .2-3% of all births • Can you predict a shoulder dystocia? • NO! most often cannot predict and occur in the absence of risk factors.
Factors that contribute to normal labour • What are the factors that contribute to normal labour? • Power • Passenger • Position
RiskFactors • Increased fetal birthweight • Increased risk with weight over 4000g. Macrosomia is >4500g. With increasing weight, risk will increase. • Post-term, excessive weight gain during pregnancy>35lbs, parity • Diabetes • Midforceps delivery • Prolonged first/second stage? • Prior shoulder dystocia • Maternal height: more risk among shorter parturients <150cm
Diagnosis • Head to body delivery time exceeding 60s • Friedman’s curve to assess labour • Abnormal labour patterns: • 1)prolonged latent phase; more than 20 hours in nulliparous or 14h in multiparous. • 2)active labour: cervix dilates less than 1cm/hour nulliparous or less than 1.2-1.5cm/hour multiparous
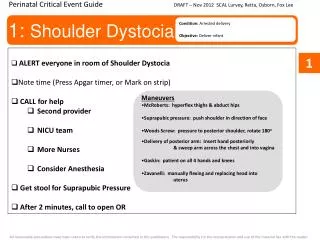
Management • Reduction maneuvers – HELPERR Mnemonic • Call for Help • Evaluate for Episiotomy • Legs (McRoberts Maneuver) • Suprapubic Pressure • Enter maneuvers (internal rotation) • Removal of the posterior arm • Roll the patient
Management • Reduction maneuvers – HELPERR Mnemonic • What we’re trying to accomplish: • Increase functional size of the bony pelvis • Decrease the bisacromial diameter (breadth of the shoulders) • Change the relationship of the bisacromial diameter within the bony pelvis
Management http://www.youtube.com/watch?v=j_bibDLPW98&noredirect=1
Management • If those maneuvers fail: • Last resort: • Deliberate clavicule fracture • Zavanelli maneuver • General anesthesia • Cesarian section • Symphysiotomy
Prophylactic management • Typically, you can’t predict, so you can’t prevent! • (ACOG) Task Force on Neonatal Brachial Plexus Palsy clinical situations as high risk for shoulder dystocia and brachial plexus injury: • Estimated fetal weight >5000 g in women without diabetes or >4500 g in women with diabetes • Prior shoulder dystocia, especially with a severe neonatal injury • Midpelvicoperative vaginal delivery of a fetus with estimated weight >4000 g *Cesarean section is a reasonable option for these patients, but is discussed as a case by case basis.
Complications • Remember: diagnosis and timing are key • Why? • Avoid complications: • Fetal: • Asphyxia • Cortical injury due to cord compression and asphyxia • Transient/permanent brachial plexus palsy • Clavicular or humeral fracture • Death • Maternal: • Hemorrhage • Fourth degree lacerations
Clinical case: Shoulder dystocia • A 30 yo G2P1 is delivering at 41 weeks gestation. She is moderately obese, but the fetus appears to clinically weigh approximately 3700 g. After a 4-hour first stage of labor and 2-hr second stage of labor, the fetal head delivers but is noted to then retract back toward the patient’s introitus (turtle sign). The fetal shoulders do not deliver, despite strong maternal pushing. • Diagnosis • Risk Factors • Management Principles of this Obstetric Emergency/ Initial Maneuvers to manage this condition • Review Neonatal and Maternal Complications of this event
Case discussion • fetal weight (passenger) estimation is inaccurate. If weight is greater than 4000-4500g the risk of dystocia including shoulder dystocia and fetopelvic disproportion is greater. Fetal macrosomia defined as birthweight over 4500g(ACOG) • 2 hour second stage- for multiparas we limit to one hour or 2 hours with regional analgesia- for nulliparas limit to 2 h or 3 h with regional analgesia • Rates of chorioamnionitis, PPH, instrumental delivery, Cesarean section and perineal trauma increase with increasing length of the active second stage of labour. • What is significance of turtle sign? May herald shoulder dystocia • Risk factors in this case : maternal obesity, pelvis ?- anatomy unknown (mother is G2 but first baby premature). No prior history of dystocia in this case. No history of diabetes. Mother’s height unknown.
References • Baxley, E; Gobbo, R. Shoulder Dystocia 2004 American Family Physican, 69(7), p. 1707-1714 • Beckmann et al. Obstetrics and Gynecology. 7th edition 2014 Lippincottt Williams & Williams. • Uptodate.com