Download
1 / 38
390 likes | 605 Views
The Neuromuscular Junction ( Neuromuscular Synapse ). Dr. Taha Sadig Ahmed. Anterior Horn Cells ( Motor Neurons ). Motor Unit : is the motor neuron (Anterior horn Cell) and all the muscle fibers it supplies. Neuromuscular Junction (NMJ). The Neuromuscular junction consists of.

E N D
The Neuromuscular Junction( Neuromuscular Synapse ) Dr. Taha Sadig Ahmed
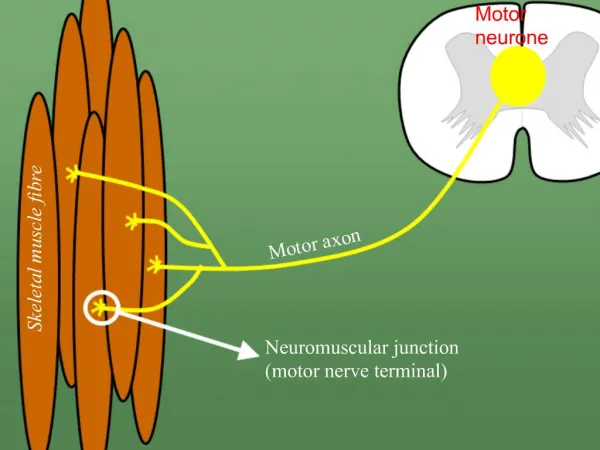
Motor Unit : is the motor neuron (Anterior horn Cell) and all the muscle fibers it supplies
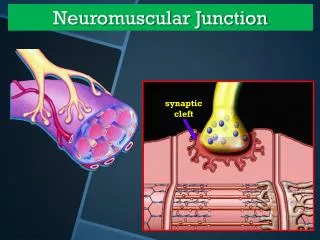
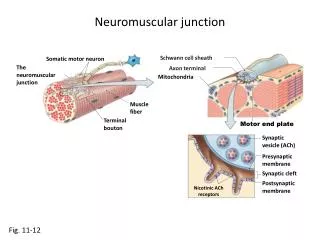
The Neuromuscular junction consists of A/ Axon Terminal : contains around 300,000 vesicles which contain the neurotransmitter acetylcholine (Ach). B/ Synaptic Cleft : 20 – 30 nm ( nanometer ) space between the axon terminal & the muscle cell membrane. It contains the enzyme cholinesterase which can destroy Ach . C/ Synaptic Gutter ( Synaptic Trough) It is the muscle cell membrane which is in contact with the nerve terminal . It has many folds called Subneural Clefts , which greatly increase the surface area , allowing for accomodation of large numbers of Ach receptors . Ach receptors are located here .
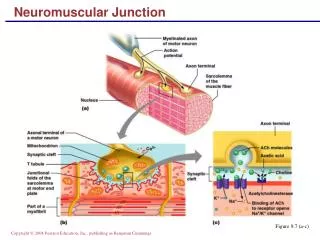
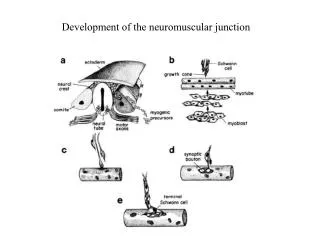
The Neuromuscular junction consists of • The entire structure of axon terminal , synaptic cleft and synaptic gutter is called “ Motor End-Plate ” . • Ach is synthesized locally in the cytoplasm of the nerve terminal , from active acetate (acetylcoenzyme A) and choline. • Then it is rapidly absorbed into the synaptic vesicles and stored there. • The synaptic vesicles themselves are made by the Golgi Apparatus in the nerve soma ( cell-body). • Then they are carried by Axoplasmic Transport to the nerve terminal , which contains around 300,000 vesicles .
Ach is synthesized locally in the cytoplasm of the nerve terminal , from active acetate (acetylcoenzyme A) and choline. Then it is rapidly absorbed into the synaptic vesicles and stored there. The synaptic vesicles themselves are made by the Golgi Apparatus in the nerve soma ( cell-body). Then they are carried by Axoplasmic Transport to the nerve terminal , which contains around 300,000 vesicles . Each vesicle is then filled with around 10,000 Ach molecules . Acetylcholine (1)
When a nerve impulse reaches the nerve terminal , it opens calcium channels calcium diffuses from the ECF int the axon terminal Ca++ releases Ach from vesicles by a process of EXOCYTOSIS One nerve impulsecan release 125 Ach vesicles. The quantity of Ach released by one nerve impulse is more than enough to produce one End-Plate Potential . Acetylcholine (2)
Ach combines with its receptors in the subneural clefts. This opens sodium channels & sodium diffuses into the muscle causing a local,non-propagated potential called the “End-Plate Potential (EPP)”, whose value is 50 – 75 mV. • This EPP triggers a muscle AP which spreads down inside the muscle to make it cntract .
After ACh acts on the receptors , it is hydrolyzed by the enzyme Acetylcholinesterase (cholinesterase ) into Acetate & Choline . The Choline is actively reabsorbed into the nerve terminal to be used again to form ACh. This whole process of Ach release, action & destruction takes about 5-10 ms .
Myasthenia Gravis • Auto-immune disease • Antibodies against Ach receptors destroy many of the receptors decreasing the EPP , or even preventing its formation weakness or paralysis of muscles ( depending on the severity of the disease ) . • patient may die because of paralysis of respiratory muscles. • Treatment : Anti-cholinestersae drugs . These drugs inactivate the cholinesterase enzyme ( which destroys Ach) and thereby allow relatively large amounts of Ach to accumulate and act on the remaining healthy receptors good EPP is formed muscle contraction .
Drugs Acting on the NMJ • Drugs that stimulate the muscle cell by Acetylcholine-like action : nicotine , methacholine , carbachol . • Drugs that block neuromuscular transmission : Curare and curare-like drugs ( curariform drugs ) . They have a chemical structure similar to ACh , but can not stimulate the receptors . They occupy acetylcholine receptors and thereby prevent ACh from acting on its receptors muscle weakness or paralysis . Example : Tubocurarine. It is used during some surgical operations . • Anticholinesterase drugs ( e.g. Neostigmine,Physostigmine) Used in treatment of Myasthenia Gravis . These drugs inactivate the cholinesterase enzyme ( which destroys Ach) and thereby allow relatively large amounts of Ach to accumulate and act on the remaining healthy receptors good EPP is formed muscle contraction .
The Muscle Action Potential • Muscle RMP = -90 mV ( same as in nerves ) . • Duration of AP = 1-5 ms ( longer duration than nerve AP , which is usually about 1 ms ) . • CV = 3-5 m/s ( slower than big nerves ) .
Muscle Contraction There are 4 important muscle proteins : A/ two contractile proteins that slide upon each other during contraction: • Actin • Myosin , B/ And two regulatory proteins : • Troponin excitatory to contraction • Tropomyosin inhibitory to contraction
Each muscle cell (fiber) is 10 -80 micrometer long & is covered by a cell-membrane called Sarcolemma. • Each cell contains between a few hundreds to a few thousands Myofibrils. • Each Myofibril contains 3000 Actin filaments & 1500 Myosin filaments . • Each myofibril is striated: consisting of dark bands (called A-bands) and light (I-bands).
Muscle Structure (2) • A-bands consist mainly of Myosin & Actin ; while I-bands consist of Actin. • The ends of Actin are attached byZ-Discs(Z-lines ). • The part of the Myofibril lying between two Z-discs is called Sarcomere . It is about 2 mcrometers . • When contraction takes place Actin & Myosin slide upon each other , & the distance between two z-discs decreases : This is called Sliding Filament Mechanism
Actin Filament consists of Globular G-actin molecules that are attached together to form a chain. Each two chains wind togetherاlike a double helix Two F-Actin strands Groove between the 2 F-actin strands
> Each G-Actin molecule has a binding site for Myosin head( called actin active sites ) > These active sites are covered and hidden from the Myosin head by the inhibitory protein Tropomyosin > When Troponin is activated by Ca++ it will move the Tropomyosin away from these sites and expose them for Myosin.> then myosin immediately gets attached to them .> when the myosin head attaches to actin it forms a “ cross-bridge”
Myosin (1) • Each Myosin molecule has (1) Head (2) Hinge (joint ) and ( 3 ) Tail ; and each myosin head contains an ATP binding site as well as ATP-ase enzyme .
Myosin (2) • Each 200 myosin molecules aggregate to form a myosin filament , from the sides of which project myosin heads in all directions .
The EPP at the motor end-plate triggers a muscle AP The muscle AP spreads down inside the muscle through the Transverse Tubules ( T-tubules ) to reach the Sarcoplasmic Reticulum (SR) . In the SR the muscle AP opens calcium channels ( in the walls of the SR) calcium passively flows out ( by concentration gradient ) of the SR into muscle cytoplasm Ca++ combines with Troponin
The activated troponin pulls the inhibitory protein tropomyosin away from the myosin binding sites on actin and once these sites on Actin are exposed myosin heads quickly bind to them
This binding activates the enzyme ATPase in the Myosin Head it breaks down ATP releasing energy which is used in the “Power Stroke ” to move the myosin head
The “ power stroke ” means tilting of the cross-bridge head ( myosin head ) and dragging ( pulling ) of actin filament
Then , on order to release the head of Myosin from Actin , a new ATP is needed to come and combine with the head of Myosin . • Q: What is Rigor Mortis ? • Q: ATP is neede for 3 things : what are they ? • Q: Is muscle relaxation a passive or active process ? Why ? • Q: What happens to A-band and I-band during contraction ? • Q: Ca++ is needed in nerve & muscle : when and where ?
Summary (1) • Muscle AP spreads through T-tubules • it reaches the sarcoplasmic reticulum where opens its Ca++ channels calcium diffuses out of the sarcoplasmic reticulum into the cytoplasm increased Ca++ concentration in the myofibrillar fluid . • Ca++ combines with Troponin , activating it • Troponin pulls away Tropomyosin • This uncovers the active sites in Actin for Myosin • Myosin combines with these sites • This causes breakdown of ATP and release of snergy which will be used in Power Stroke • Myosin and Actin slide upon each other contraction • A new ATP comes and combines with the Myosin head .This causes detachment of Myosin from Actin .
Summary (2) • ATP is needed for 3 things : • (1) Power stroke . • (2) Detachment of myosin from actin active sites . • (3) Pumping C++ back into the Sarcoplasmic reticulum .
Cardiac Muscle (1) • Cardiac muscle is a type of highly oxidative (using molecular oxygen to generate energy ) involuntary striated muscle found in the walls of the heart, • Cardiac muscle is adapted to be highly resistant to fatigue: it has a large number of mitochondria, enabling continuous aerobic respiration via oxidative phosphorylation, • Role of calcium in contraction • In contrast to skeletal muscle, cardiac muscle requires both extracellular calcium and sodium ions for contraction to occur.
Cardiac Muscle (2) • Like skeletal muscle, the depolarization phase of the ventricular muscle action potential is due to entry of sodium ions across into the cell . • However, an inward flux ( influx ) of extracellular calcium ions through calcium channels sustains the depolarization of cardiac muscle cells for a longer duration , resulting in a “ plateau Phase ” that is not present in the case of the skeletal muscle AP • Therefore , the cardiac muscle AP lasts for a long period ( 200-2300 ms ) and covers most of the contraction phase . That is why cardiac muscle can not be tetanized . • Repolarization in the AP , like skeletal muscle , is due to potassium efflux .
Phase 4 Phase 4 is the Resting Membrane Potential . The normal resting membrane potential in the ventricular myocardium is about -85 to -95 mV. This is the period that the cell remains in until it is stimulated by an external electrical stimulus (typically an adjacent cell). This phase of the action potential is associated with diastole ( relaxation ) of the chamber of the heart Phases of the Cardiac Muscle AP (1)
Phase 0: Phase 0 is the rapid depolarization Phase 1: Phase 1 of the action potential occurs with the inactivation of the sodium channels . Phases of the Cardiac Muscle AP (2)
Phase 2 Phase 2 is the "plateau" phase of the cardiac AP and is due to calcium influx into the cell . Phase 3 Phase 3 is the repolarization phase and is due to potassium efflux Phases of the Cardiac Muscle AP (3)
Draw the relationship between a cardiac AP and cardiac muscle contraction. How does this situation compare to excitation contraction coupling of skeletal muscle? • In skeletal muscle, the electrical event is over before the contraction begins, • but in cardiac muscle, the electrical and mechanical eventsoverlap considerably. • Tetany is not possible in cardiac muscle because of the prolonged refractory period.