Download
1 / 46
480 likes | 666 Views
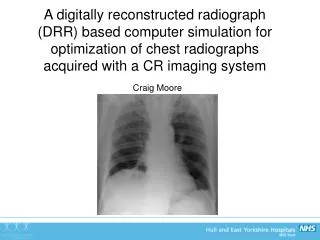
Optimisation of Computed Radiography chest imaging utilising a digitally reconstructed radiograph simulation technique. Craig Moore Radiation Physics Service Hull & East Yorkshire Hospitals NHS Trust www.hullrad.org.uk. Introduction - Literature.

E N D
Optimisation of Computed Radiography chest imaging utilising a digitally reconstructed radiograph simulation technique Craig Moore Radiation Physics Service Hull & East Yorkshire Hospitals NHS Trust www.hullrad.org.uk
Introduction - Literature • Lots of publications have shown that patient anatomy is the limiting factor in the reading normal structures, and detection of lesions (lung nodules) in chest images • Bochud et al 1999 • Samei et al 1999, 2000 • Burgess et al 2001 • Huda et al 2004 • Keelan et al 2004 • Sund et al 2004 • Tingberg et al 2004 • European wide RADIUS chest trial (2005)
Introduction - Literature • Chest radiography is now generally considered to be limited by the projected anatomy • Patient anatomy = anatomical noise So if we want to optimize digital system for chest imaging, vital that anatomical noise is present in the images!!!
Introduction • However, the radiation dose/image quality relationship must not be ignored • Doses must be kelp ALARP • ICRP 2007 • IR(ME)R2000 – (required legally in the UK) • We would therefore want system (quantum) noise present in an image for dose reduction studies
Digitally Reconstructed Radiograph (DRR) • Hypothesis: • Can use CT data of humans to provide realistic anatomy (anatomical noise) • Clinically realistic computerized ‘phantom’ • Simulate the transport of x-rays through the ‘phantom’ and produce a digitally reconstructed radiograph (DRR – a simulation of a conventional 2D x-ray image created from CT data) • Add frequency dependent system noise post DRR calculation • Add radiation scatter post DRR calculation • Validate • Use for optimization studies
DRR Algorithm: Virtual Patient • Virtual patient derived from chest portion of real CT datasets • Voxel resolution = 0.34 x 0.34 x 0.8 mm • CT number converted to linear attenuation coefficient (LAC) using tissue equivalent inserts • Measure mean CT No. in each insert • We know elemental composition of each so can derive LAC • Can derive relationship between CT No. and LAC
Energy absorbed in CR phosphor Final CT axial batch (i.e. slices 681 to 700) CT axial batch 2 (i.e. CT slices 21 to 40) PA slice N CT axial batch 1 (i.e. CT slices 1 to 20) PA slice 1 CT dataset re-orientated in the ‘PA’ direction Intensity of X-rays exiting is calculated X-ray attenuated exponentially through CT dataset using a ray casting method of DRR calculation X-ray spectra derived from IPEM 78
Scatter Addition • Must add to DRR generated image • DRR algorithm does not calculate scatter • Measured scatter in CR chest images using lead pellet array • Use chest portion of RANDO phantom
Noise Addition Based on slightly modified work by Bath et al, 2005 lung spine diaphragm Corrected noise image Uniform noise image
Lung Nodule Simulation • Added artificial nodules to the CT data prior to X-ray projection • Baed on work by Li et al 2009
Human DRR v Human CR DRR CR
CR DRR DRR (c) (a) (b) Scatter Rejection • The DRR algorithm can produce images with scatter rejection DRR No Rejection DRR Grid CR Grid
DRR CR (a) (b) Obese Patients • DRR algorithm can also produce images of large/obese patients
Validation • Decided to validate with RANDO and real patient images: • Histogram of pixel values • Signal to noise ratios (SNR) • Important because signal and noise affects the visualisation of pathology • Tissue to rib ratios (TRR) • Pixel value ratio of soft tissue to that of rib • Important as rib can distract the Radiologist from detecting pathology
a c b d Phantom Histograms
PATIENT - Histograms Typical histogram of average patient DRR Typical histogram of average patient CR image
SNRs • Good agreement in lung, spine and diaphragm areas of chest • Maximum deviation approx 15% • Mean deviation = 7% • Addition of frequency dependent noise not perfect: • CR system noise is ergodic (changes with time) • Noise added here is a snapshot (and so not ergodic) • However, quantum noise dominates over ‘ergodic noise’ so not such an issue • DQE is NOT constant with dose variation in image
Validation - TRRs • Good agreement • Within 2% • As tube potential increases TRR decreases • Due to rib attenuating higher percentage in incident photons at lower potentials than soft tissue, thus forcing up TRR
Validation - Radiologists • Have told me DRR images contain sufficient clinical data to allow diagnosis and subsequent optimisation • They have scored the images out of 10 • ‘are the images sufficiently like real CR images? • Average score of 7.8
Conclusions – DRR Algorithm • DRR computer program has been produced that adequately simulates chest radiographs of average and obese patients • Anatomical noise simulated by real human CT data • System noise and scatter successfully added post DRR generation that provides: • SNRs • TRRs • Histograms • in good agreement with those measured in real CR images • Provides us with a tool that can be used by Radiologists to grade image quality with images derived with different x-ray system parameters • WITHOUT THE NEED TO PERFORM REPEAT EXPOSURE ON PATIENTS • ACCEPTED FOR PUBLICATION IN THE BJR • AUGUST 2011
Optimisation of CR Chest Radiography using DRR Generated Images • In Hull chest exposure factors were not standardised (historical reasons!!!!) • Three main hospital sites: • 60 kVp & 10 mAs • 70 kVp & 5 mAs • 80 kVp & 5 mAs • In the last 6 months, four expert image evaluators have scored DRR reconstructed images • Two Consultant Radiologists • Two Reporting Radiographers • Scoring criteria based on European guidelines (CEC)
What to Optimise? • Optimum tube potential for Average Patients (70 kg ± 10 kg) • Without scatter rejection (as per Hull protocol) • With scatter rejection (grid and air gap) • Optimum tube potential for Obese patients • Without scatter rejection • With scatter rejection • Is Scatter rejection indicated? • Dose reduction?
Scoring Criteria • Images scored on a dual PACS monitor system • Image on right hand screen held at a constant kVp • Images on left hand screen displayed from 50 to 150 kVp in steps of 10kVp (approx) • Image 1 = 50 kV • Image 2 = 60 kV • Image 10 = 150 kV • Test images scored against reference image • All images matched effective dose
[1] European guidelines on quality criteria for diagnostic radiographic images. CEC European Commission EUR 16260 EN (Luxembourg 1996)
Results – Average Sized Patients, no scatter rejection VGAS = average of Radiologists results
Results – Obese Patients without scatter rejection • Very weak trend for better image quality with higher kVp • Lower kVps probably ‘worse’ due to combination of: • Lack of penetration through obese patient • Increased scatter from obese patient (scatter to cassette changes very little with kVp) • This is not so with average patients • Less tissue (fat) so more radiation penetration • Less scatter from fat • It is likely that poorer radiation penetration and increased scatter from obese patient outweighs the inherent benefit of photoelectric contrast obtained from lower kVps
Scatter Rejection vs no scatter rejection – average patients
Scatter Rejection vs no scatter rejection – average patients • Superior image quality with scatter rejection technique • Grids performed much better than air gap • Statistically significant differences • BUT: • Image evaluators were asked if increase in dose due to use of grids was justified, even with better image quality • Answer in 100% of cases was NO • SCATTER REJECTION FOR AVERAGE PATIENTS IS NOT INDICATED
Exposure time for average patients without scatter rejection and low tube potentials? • Scatter rejection not indicated • Therefore low kVps should be used (remember the graph) • European guidance recommends exposure times < 20 ms • Can we achieve this with low kVps?? • Modern Philips X-ray generator: • For lgM = 2 (Agfa CR specific Dose Indicator) • With 630 mA, all kVps are possible • Max exp time = 16 ms • At the expense of increased tube loading
Scatter Rejection vs no scatter rejection – obese patients • Superior image quality with scatter rejection technique • Grids performed much better than air gap • Statistically significant differences • BUT: • Image evaluators were asked if increase in dose due to use of grids was justified, even with better image quality • Answer in 100% of cases was YES • ANTI SCATTER GRID USE FOR OBESE PATIENTS IS INDICATED
Exposure times for obese patients with an anti-scatter grid • Remember that low tube potentials were superior with an anti-scatter grid!!!! • Need exposure times < 20ms • Is this possible with low kVps and scatter grid for lgM = 2?? • Scatter grid is a focused grid so have to use it in a fixed range of FDD • Nominal distance = 140 cm FDD • Range allowed = 115cm – 180cm • At 140 cm FDD lowest exp time = 17.6ms @ 109 kVp • At 115cm FDD lowest exp time = 20 ms @ 90 kVp • So are limited to 90 kVp
Dose Reduction? • Images were also presented at different doses
Dose reduction? • Results suggest doses can be reduced by around 50% before image quality begins to suffer and become unacceptable • Therefore could half exposure mAs
Conclusions – Use of DRR algorithm to optimise CR chest imaging • Average patients: • No scatter rejection is indicated • Therefore, low kVps (< 102 kVp) are indicated • Can have exposure times < 20 ms for all kVps • Obese patients • Anti-scatter grid is indicated • So low kVps (<102kVp) should be used • For exposure times < 20ms, are limited to 90 kVp • Doses • As low as 50% reduction possible • ACCEPTED FOR PUBLICATION IN BJR
Optimisation & Standardisation in Hull? • Agreed with Consultant Radiologists: • 60 kVp & 10 mAs • After a ‘settling in’ period: • 60 kVp & 8 mAs • Want to go lower than 8mAs eventually!!! • Implication on patient dose? • Using PCXMC effective dose calculation software: • 80 kVp/5 mAs = 0.011 mSv • 60 kVp/8 mAs = 0.006 mSv • Approx 45% drop in effective dose