Download
1 / 14
190 likes | 850 Views
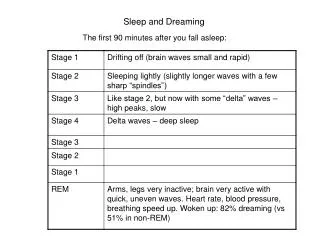
CASE PRESENTATION: Uncontrolled ‘Essential’ Hypertension, Stage II. Jasjot Garcha MD PGY1, Internal Medicine Allan B. Schwartz, MD Professor of Medicine Division of Nephrology and Hypertension Director of CME, Department of Medicine Drexel University College of Medicine.

E N D
CASE PRESENTATION:Uncontrolled ‘Essential’ Hypertension, Stage II Jasjot Garcha MD PGY1, Internal Medicine Allan B. Schwartz, MD Professor of Medicine Division of Nephrology and Hypertension Director of CME, Department of Medicine Drexel University College of Medicine
Chief Complaint and HPI: A 55 year old Caucasian male, • history of hypertension for 30 years with poor follow up and irregular BP monitoring. Pt. was diagnosed of hypertension at the age of 25 years (160/96). He was treated originally with Serapes (Reserpine + Hydralazine + HCTZ) followed by Propanolol and Triamterene/HCTZ. • presents at the nephrology clinic with a nose bleed and accompanied blood pressure of 180/110mm Hg. • ROS was within normal limits except for knee pain which is relieved by Ibuprofen.
Past medical and surgical history: • Paroxysmal atrial tachycardia with hypokalemia( 2.9 mEq/L) in his mid 20s.
Family history • Father: Died at 75 of Acute M.I. Hypertensive since his 20s with history of paroxysmal atrial tachycardia and paroxysmal atrial flutter. • Paternal Grand Father died at 81 of CHF , CAD
Social history • Physician • Runs 4 miles per day • Non smoker • occasional alcohol consumption
Medications: • Felodipine 2.5mg QD • Metoprolol 50mg BID • Triamterene/HCTZ (37.5/25) 1 tablet daily • Ibuprofen 600 mg PRN
Physical exam: • BP:160/90 mm Hg P: 50/min • Fundi show diffused arteriolar narrowing and AV nicking. • Heart: regular, No m/g • Lungs clear • Pulses intact
Labs and further studies(11/1997): • BUN/Cr:30/1.9 • TG 323, Total Chol 232, LDL 136, HDL 31 • No proteinuria • CrCl(Cockcroft Gault) = 45 ml/min • ECG: normal • Echocardiogram: no LVH • Renal scan: 8.6cm right & 9.3cm left • Renal blood flow scan: no evidence of RAS • Serum Cortisol and Aldosterone levels: Normal
Further plan: • Low salt diet • Maintain exercise program • Start Quinapril 5mg QD • Conitinue Metoprolol 50 mg BID & Triamterene/HCTZ 37.5/25 mg QD • 24 hr. urine for VMA, catecholamines, metanephrines • Consider statin
Questions: • What is the likely etiology? • How do genetics and the patient risk factors relate? • How many anti-hypertensives drugs will this patient require? • Would this patient have required a statin irrespective of his lipid profile? • What are the endothelial protective effects of statins in the hypertensive patients?
Follow up over the next 5 years : • Negative:24 hr Urine VMA, metanephrines and catecholamines • Started Amlodipine 5mg QD(7/1998) but D/C as patient felt dizzy after running (BP: 128/70) • Started Atorvastatin 10mg QD(8/1998) and ASA 81 mg QD(8/1999) • Increase Quinapril to 20mg BID (11/97-8/98)
Most Recent Labs and BP(02/2004): • BP 160/90 • BUN/Cr: 29/1.8 • TG 178, Total Chol 172, LDL 100, HDL 36 • No proteinuria • CrCl (Cockcroft Gault)= 47ml/min • ECG: normal • Echocardiogram: no LVH
Current medications: • Quinapril 20mg BID • Metoprolol 50 mg BID • Triamterene/HCTZ 37.5/25 mg QD • Atrovastatin 10mg QD • ASA 81 mg QD
Questions: • What are the reasons for the loss of BP control at this stage?