Download
1 / 27
270 likes | 304 Views
Subclinical Thyroid Disease: Where Are We Now. Dr Praveen Shankar MD, MRCP(UK). Definitions. Subclinical Disease The presence of a disease without obvious symptoms Usually indicates early stage in evolution of a disease Subclinical thyroid disease A biochemical diagnosis

E N D
Subclinical Thyroid Disease: Where Are We Now Dr Praveen Shankar MD, MRCP(UK)
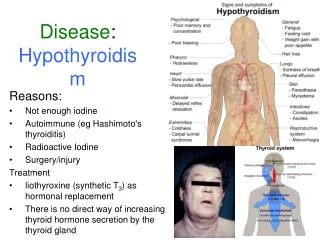
Definitions Subclinical Disease • The presence of a disease without obvious symptoms • Usually indicates early stage in evolution of a disease Subclinical thyroid disease • A biochemical diagnosis • Subclinical hyperthyroidism • ↓ TSH • ↔ FT4 & TT3 • Subclinical hypothyroidism • ↑TSH • ↔ FT4 & TT3.
How does Subclinical Thyroid Disease develop? • TSH secretion is very tightly controlled by T4 & T3 • Very small changes in serum T4 & T3 concentrations have large effects on TSH secretion • Log/linear relationship between serum TSH & FT4 • alterations in serum FT4 that is within normal range can cause increase/decrease in serum TSH concentrations that can be outside its reference range. JCEM 2002; 87: 1068–72 JCEM2004; 89: 1181–87.
Subclinical Hyperthyroidism • With mildly suppressed TSH concentrations (TSH 0.1 to 0.4 mU/L) • With completely suppressed TSH concentrations (TSH < 0.1 mU/L) • With progressive decline in TSH level chances of clinically significant consequences rises • In any population mild subclinical hyperthyroidism is more common • The population prevalence of subclinical hyperthyroidism higher in • Women • Old age • Geographical region with iodine-deficiency.
Subclinical Hyperthyroidism • Exogenous disease more common than endogenous form • 20-40% of patients on LT4 replacement have low TSH concentration • Reversible on lowering doses • Graves’ disease is the most common cause in young patients • Toxic adenoma/MNG most common cause in elderly • MNG is more typically associated with subclinical hyperthyroidism than Graves’ disease • In one study, about 20% of patients with Graves’ disease had a chronically suppressed TSH after a course of ATD or surgery , and were more likely to relapse than a comparable group with normal TSH levels. Acta Endocrinol (Copenh) 1990; 122: 623.
Progression to overt hyperthyroidism in people with completely suppressed TSH concentrations is higher Am J Med Sci 2009; 337: 225–32.
Natural History www.thelancet.com Published online January 23, 2012 DOI:10.1016/S0140-6736(11)60276-6.
Systemic effects • Similar to that of overt hyperthyroidism Bone & mineral metabolism • ↑ bone resorption • Cortical bone is affected more than trabecular bone • ↓BMD in postmenopausal women, but, little effect in men or premenopausal women • ?Whether this translates into increased risk of fracture in postmenopausal women. Atrial fibrillation • ↑ risk • Risk similar whether TSH <0.1 or 0.1-0.4 mU/L • Prevalence similar to that in overt hyperthyroidism • May remit with ATD therapy.
Systemic effects Cardiovascular system • ↑ heart rate & atrial premature beats • ?↑LV mass • Changes in coagulation indicators • ↑carotid intima-media thickness • ↑atherosclerotic CV events & CV morbidity & mortality especially in elderly patients & those with underlying cardiac disease Cognitive dysfunction & quality of life • Associated with dementia in elderly people • Palpitations, heat intolerance & anxiety cause reduction in quality-of-life scores.
Prevention of Exogenous subclinical hyperthyroidism important • Cause substantial morbidity especially in older patients • ↓BMD • ↑risk of AF • Important to carefully titrate LT4 doses to maintain normal TSH level in those on replacement therapy • TSH suppressive therapy to decrease goitre or thyroid nodule size is no longer recommended • Less aggressive TSH suppression has been suggested for patients • With low-risk thyroid cancer • Older patients who have been shown to be disease-free on follow up. Thyroid 2009; 19: 1167. Thyroid 2010; 20: 135.
Who deserve treatment? Werner & Ingbar’s The Thyroid- A Fundamental and Clinical Text 10th Edition: p520.
www.thelancet.com Published online January 23, 2012 DOI:10.1016/S0140-6736(11)60276-6.
Subclinical hypothyroidism • Biochemical diagnosis, by definition can not be identified on the basis of signs & symptoms • Consensus lacking on the upper limit of normal for serum TSH • National Academy of Clinical Biochemistry Laboratory Practice Guidelines, 2003 recommendation (endorsed by AACE ) – 2.5 mU/L • Present data support the need for age-based normal ranges for serum TSH • Consideration of TSH measurement method is important • Immunometric assay (IMA) using nonisotopic (chemiluminescent or fluorescent ) technique (3rd generation) commonly give upper limit of normal as less than 4.5 mU/L.
TSH distribution curve shifts to higher TSH concentrations with age (NHANES III & NHENES 1999-2002 databases for thyroid disease-free subjects) Potential for misclassification of older individuals as having subclinical hypothyroidism if age-specific TSH cut-off values not employed JCEM 2007; 92: 4575-82.
Prevalence • Higher in • ? Old age • White compared to black • Area with higher compared to lower, but not deficient, intake of iodine • Patients with Down syndrome, Turner’s syndrome, T1DM & possibly other autoimmune diseases, family history of autoimmune thyroid disease, endocrine or systemic autoimmune disorders • In a survey of pregnant women in the US, 2% had subclinical hypothyroidism and 58% had high anti-TPO antibody concentration.
Systemic effects Cardiovascular effects • Subclinical hypothyroidism is associated with hypercholesterolemia, atherosclerosis and other CV changes like ↑SVR & arterial stiffness, altered endothelial function & coagulability • ? Do they -result in adverse cardiovascular events: Conflicting data A meta-analysis of individual participant data done by Thyroid Studies collaborators • 11 prospective cohort studies • Total no. of participants 55,287 • Subclinical hypothyroidism was defined as TSH between 4.5 to 20 mU/L with normal T4 concentration.
The risk of CHD events & CV mortality, but not total mortality, increased significantly with TSH ≥ 10 mU/L
Women of reproductive age and during pregnancy • Prevalence is 0.5-5% depending on the cut-off value for TSH used to define the condition • Associated with serious obstetric complications- increased risk of miscarriage, placental abruption, preterm delivery, gestational HTN, LBW • Thyroid hormone essential for fetal brain development & maturation especially during 1st trimester of pregnancy • Impaired mental development has been reported in children born to women who were inadequately treated for subclinical hypothyroidism • The Endocrine Practice guidelines recommends treatment of subclinical hypothyroidism in pregnancy. NEJM 1999; 341: 549-55. JCEM 2012; 97:2543-65.
Neuropsychiatric health • It seems patients with autoimmune thyroid disease (majority will be subclinical hypothyroidism) have increased propensity towards depression • Patients with depression and subclinical hypothyroidism compared to those with depression & euthyroidism have • Higher prevalence of associated panic disorder • Poorer response to antidepressant drug therapy. Werner & Ingbar’s The Thyroid- A Fundamental and Clinical Text 10th Edition: p632.