Download
1 / 16
220 likes | 531 Views
By:Dawit Ayele. ACUTE RHEUMATIC FEVER. Definition. Rheumatic fever is an inflammatory disease that occurs as a delayed, non- suppurative sequela of upper respiratory infection with group A streptococci. Etiology. Antecedent infection with specific microorganism- Gp A streptococci

E N D
By:DawitAyele ACUTE RHEUMATIC FEVER
Definition • Rheumatic fever is an inflammatory disease that occurs as a delayed, non-suppurativesequela of upper respiratory infection with group A streptococci.
Etiology • Antecedent infection with specific microorganism- Gp A streptococci • At specific site- upper respiratory tract-nowhereelse • Heavily encapsulated, as evidenced by their growth as mucoid colonies on blood agar plates. • Predominant strains 3, 5, 18, 24, and others
Epidemiology • 3% of individuals with untreated gp A streptococci will develop RF. • Most often occurs in children; the peak age-related incidence is b/n 5 and 15 years. • Risk factors for outbreak: -lower standards of living esp.crowding, -the organism itself -the degree of host/herd immunity to the prevalent M-types in an affected community
Pathogenesis • Study Hypothesis of ‘antigenic mimicry’: 1)Similarity between the group-specific CHO of the gp A streptococcus & the glycoprotein of heart valves, -2)the molecular similarity among the streptococcal cell membrane, strept M ptnsarcolemma,& other moieties of human myocardial cell. • Possiblity of predisposing genetic influencedifferences in immune response to strept
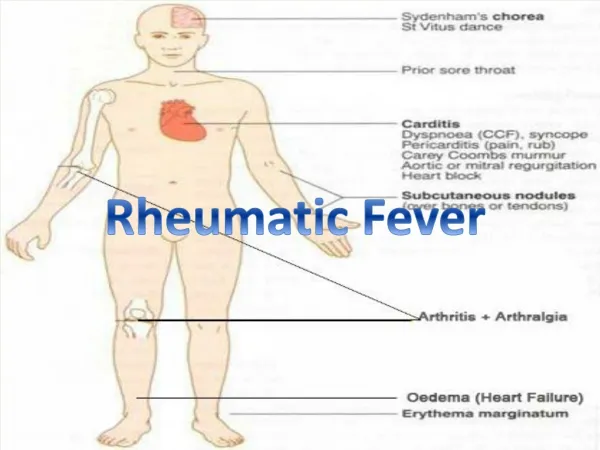
Clinical feature -- most notably affect the heart, joints, skin, subcutaneous tissue, and central nervous system. POSSIBLE FEATURES • High fever, prostration, crippling polyarthritis • Lassitude, tachycardia, new cardiac murmurs • Acute pericarditis • Fulminant heart failure • Sydenham's chorea without fever or toxicity • Acute abdominal pain mimicking appendicitis • Varying combinations of the above
Diagnosis • No specific test to establish Dx • *Clinical+supportive evidence from microbiology & clinical immunology lab • 1944 Jones proposed standard criteria • 1992 updated Jones published by AHA • To fullfill the dx requires either 2 major or 1 major & 2 minor + evidence of antecedent streptococcal infection
The Jones Criteria Major • Carditis • Migratory polyarthritis • Sydenham’s chorea • Subcutaneous nodules • Erythemamarginatum + Supporting evidence of a recent gp A strept infection(throat culture or rapid antigen /ab test ASO-80%+) Minor • Clinical-fever -arthralgia • Lab-↑acute phase reactants- (↑ ESR) -prolonged PR
Carditis • 40-60% of RF cases have evidence of carditis • Pancarditis involve- pericardium, myocardium& endocardium • Cx-sinus tachycardia, -murmur of MR -S3 gallop -pericardial friction rub -cardiomegaly 20%-subtle mitral valve abnormality w/o audible murmur(echo dx)
Carditis… • Commonly affected valves: -Mitral(pure ms or ms/mr) -Aortic-isolated is rare-mitral valve is almost always simultaneously affected -tricuspid & pulmonic –not commonly affected
Migratory Polyarthritis • In as many as 75% of cases • Extremely painful joint pain & swelling • Most often affects-ankles, wrists,knees& elbows • Not usually affected-small joints of hands or feet;seldom involves hip joints
Sydenham’s chorea • CNS d/o • <10% of patients • It may happen in as long as several months from initial strept infection
Subcutaneous nodules & erythemamarginatum • Uncommon manifestations • Nodules found over extensor surface of joints • Are seen most often in patients with long standing Rheumatic heart dis. • EM usually concentrated on the trunk as evanescent macular eruption with rounded borders
Treatment Two necessary therapeutic approach to ARF pts 1)Anti –Strept antibiotic treatment:for all patients with ARF whether culture is +/- Conventional-10 days course of oral penicillin v 5oo mg po bid or erythromycin for penicillin allergy Choise of many-Benz. Penicillin G 1.2 mill IU 2)Treatment for clinical manifestation of the disease-arthritis-ASA upto 2 gm qid -CHF –conventional medical measures -Chorea-reassurance for most-resolves in 6wks to 6 mths
2o prophylaxis • AHA recommendations- Benzanthine penicillin 1.2 million IU IM Q 4 weeks or for oral penicillin V(250mg 2x/day)or oral sulfadiazine 1 gm daily. • For those with higher risk Benz. Penicillin q 3 wks is more effective in decreasing risk of recurrence. • Risk of recurrence is highest during the 1st 5 yrs after attack—2ry prophylaxis is always given for at least these period. • Continued rx for high risk exposure gp-students,teachers,medical& military personnel. • Many believe documented recurrences &/or documented RVD should receive 20px for life!!