Download

1 / 29
290 likes | 373 Views
Genetic counselling. Mary Porteous Mary.porteous@ed.ac.uk. What is genetic counselling?.

E N D
Genetic counselling Mary Porteous Mary.porteous@ed.ac.uk
What is genetic counselling? • The process by which patients or relatives at risk of a disorder that may be hereditary are advised of the consequences of the disorder, the probability of developing or transmitting it, and of the ways in which this may be prevented, avoided or ameliorated • Peter Harper
Genetic counsellors • Clinical Geneticists • Genetic Nurse Specialists • Genetic Associates (Science graduates) • Counsellors in specific areas (Haemophilia etc) • Should all healthcare professionals be able to communicate genetic issues?
Genetic Testing • Identification of disease genotype in a family • Identification of a genetic disease in a family?
Pre-symptomatic Testing • Identification of a genotype before a phenotype develops • HD trinucleotide expansion • Identification of a marker of a disease before symptoms develop • High cholesterol in hypercholesterolaemia • Renal cysts in adult polycystic kidney disease
Is the disease worth testing for? • Can we predict the course of the disease? • Can we improve treatment? • Can we affect outcome? • Is termination of pregnancy justified?
Do we have an appropriate test? • Has the genetic change been identified? • In the condition? • In the family? • Is the test accurate and reproducible? • Is there a lab that will perform the test? • GENETIC TESTING IS NOT AVAILABLE FOR MOST SINGLE GENE DISORDERS
HD as a model for Pre-symptomatic testing • Highly sensitive and specific diagnostic test • Fully penetrant disease • Relatively consistent clinical course
Pre-enrollment appointmentPre-symptomatic testing protocol • Confirm diagnosis in affected relative • Draw up family tree • General discussion about HD
First Appointment • Discuss basis of test • Assess knowledge of HD • Review information
Second Appointment • Why are you having the test now? • What are the benefits of a result positive or negative? • Who else is likely to be affected by your result? • Check knowledge base
Third Appointment • How have you coped with major life changes in the past? • How will you get the result? • Who will you share it with? • Blood taken at this appointment
Results • A firm date for result is given when the blood is taken • Result given in clinic or at home • Contact arranged for 2-4 weeks and then negotiated
CADASIL • Autosomal dominant disease - mutations in NOTCH gene • Recurrent strokes and resulting disability • Migraine may occur 10 years before onset of strokes • Variable clinical course but penetrance nearly complete • Often associated with a characteristic MRI scan
Letter to neurologist • This 24 year old woman has been complaining of headache for the past 2 years. The headaches are associated with visual aura and vomiting. She is the main carer for her 52 year old wheelchair-bound mother.
Neurology appointment • Symptom history strongly suggestive of migraine • Family history - stroke in mother and maternal uncle • Could be CADASIL - MRI scan ordered to confirm
Letter to geneticist • This 24 year old lady has a strong family history of stroke. Her mother is wheelchair-bound at 52 and her uncle died at 47. Apart from intermittent migraine she is in good health.
Genetic Clinic Appointment • Family history suggestive of CADASIL • Migraine may be associated but also common in the general population - not necessarily symptomatic of CADASIL • Discussion of genetic testing (sample from mother to look for mutation) • Pre-symptomatic protocol explained
Discussion • Is MRI a pre-symptomatic test in this situation? • Which approach is better? • Could you combine approaches?
Why do we place so much more emphasis on gene testing compared with other clinical testing?
Treatable v non-treatable • What sort of protocol should we have for: • Huntington’s disease • Breast cancer • Bowel cancer • Polyposis coli
Hypercholesterolaemia (high blood cholesterol levels) • Some people have a dominantly inherited mutation leading to high cholesterol • Some have a genetic susceptibility to high cholesterol • We can all have high cholesterol if we don’t eat a decent diet. • Drug treatments are expensive
Is Hypercholesterolaemia a genetic problem or a social problem? • Does genetic testing have a role? • Do you eat a good diet? • If not, would genetic testing make you improve it? • Statins are a class of drug that improve outcome in all forms of hypercholesterolaemia • Should they be available to everyone or just individuals with LDL receptor mutations?
Genetic susceptibility • What would you do if you were told that your risk of developing diabetes was twice the population risk • Change diet? • Exercise? • Panic? • Nothing?
Data Protection • Confidentiality • Individual rights versus social responsibility • Who owns genetic information?
Martin (DMD) 1. • Martin was diagnosed at 2yrs with DMD following investigation for developmental delay. A dystrophin deletion is demonstrated in both Martin and his mother Sue. Sue has 2 younger sisters neither of whom is in a stable relationship. Her mother died in a car accident and there is little contact with the extended family.
Martin (DMD) 2 • Sue who has a history of depression feels very guilty about being a carrier of DMD. Her husband phones the department to say that they wish no further contact from genetics. He says Sue has told her sisters that there is a genetic test available and they are not interested but may make contact later.
Martin (DMD) 3 • Sue’s cousin Carol attends another Genetic Department after a friend tells her about the diagnosis in Martin. • How can information be shared?
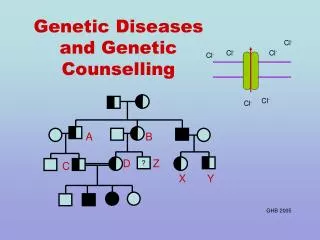
CAROL SUE MARTIN Martin (DMD)