Download
1 / 18
180 likes | 346 Views
Revascularisation coronaire. Revascularisation coronaire Veines. Saphène interne > saphène externe (v. céphalique) moins adapté à celui des artères coronaires. Perméabilité à 10 ans: -Globale :50%-60%. -IVA: 80%. Revascularisation coronaire Artère mammaire interne.

E N D
Revascularisation coronaireVeines • Saphène interne > saphène externe (v. céphalique) • moins adapté à celui des artères coronaires. • Perméabilité à 10 ans: -Globale :50%-60%. -IVA: 80%.
Revascularisation coronaireArtère mammaire interne • Prélevée sans incision supplémentaire. • Conduit à paroi élasto-musculaire. • Fonction endothéliale :ERF+Prost. • Perméabilité à 10 ans : ~90%(IVA). • Perméabilité à 5 ans: -AMIG :> 95% -AMID :~ 90%
Revascularisation coronaireArtère radiale • Prélèvement facile. • Disponibilité ≥ 90%. • Matériel agréable. • Conduit musculaire spasme. • Perméabilité :(+ inhibiteur Ca) -1 an :97%. -5 ans :~ 85%.
Age Physiologique > 75 ans < 65 ans 65-75 ans Facteurs de risque Conduits veineux Conduits veineux A.mammaires Conduits artériels Conduits mixtes Conduits veineux Allen Allen A. mammaire A. radiale Conduits mixtes A.mammaires A. mammaire A. radiale Revascularisation coronaireChoixdu conduit - + + - + - + + -
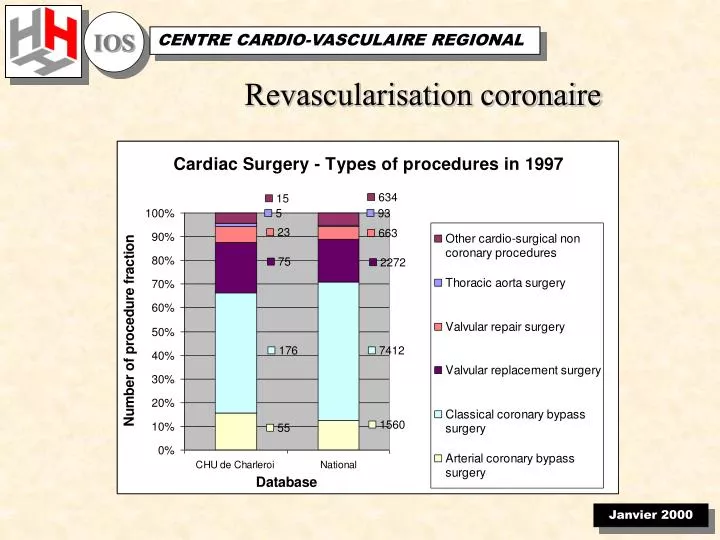
Total coronary revascularization with the internal thoracic arteries T graft C.H.U. de Charleroi
Total coronary revascularization with the internal thoracic arteries T graft • 1960 : RITA RCA • 1965 : LITA LAD • 1973 : RITA + LITA in situ • 80’s : LITA on LAD improves long-term survival
Total coronary revascularization with the internal thoracic arteries T graft • Sternal infection risk factors • Univariate analysis : • bITA grafting • Obesity • Diabetes • Prolonged mechanical ventilation • Multivariate regressive analysis : • bITA grafting p=0.0001 • Obesity p=0.0014 • Prolonged ventilation p=0.0018 Kouchoukos. Ann. Thorac. surg. 1990
Total coronary revascularization with the internal thoracic arteries T graft • ITAs have proved to be the best bypass graft but have an inadequate length to bypass Cx pl and RC arteries to achieve a complete revascularization.
Total coronary revascularization with the internal thoracic arteries T graft • Material:( jan. 94 - sept. 97 ) • 106 patients , 1/10 • Age: 51 ys (35-69) • Redo: 8 % • Diabetes: 21% • Obesity: 38 %
Total coronary revascularization with the internal thoracic arteries T graft • Material: • NYHA: II: 49 % • III: 13 % • IV: 22 % • Stress test: 58 patients. • 90 % • EF: 0.60 (0.22-0.85) +
Total coronary revascularization with the internal thoracic arteries T graft
Total coronary revascularization with the internal thoracic arteries T graft • Operative data: • Anastomoses: 4.25 (3-6) • 3 (2-4) redo patients. • Aortic cross clamping: 94 ±18 min. • IABP: 1 (EF:0.25) • Exploration for bleeding: 0
Total coronary revascularization with the internal thoracic arteries T graft • Morbidity: • Transient s-t elevation: 12 (11 %) • Q wave infarction: 3 (3 %) • Sternal infection: 1 (1%) • Mortality: 0
Total coronary revascularization with the internal thoracic arteries T graft • Follow-up(105 patients) • 35 months(15-61) • Survival: 99 % • Stress test:80 patients. • 90 % • Recurrent angina: 7 NYHA II (7 %) • infarct: 0 • Sternal instability: 2 % rewiring -
Total coronary revascularization with the internal thoracic arteries T graft • Has the potential to increase event-free survival and reduce the need for reoperation in patients with three-vessel disease. • Can be performed with a low mortality and morbidity in a selected population, even in patients requiring reoperation. • Good experience in ITA grafting is essential to the success of the procedure, especially in redo operations.
Total coronary revascularization with the internal thoracic arteries T graft FAQs • Is the blood supply sufficient? • clinical results . • Experimental studies. • What about subclavian artery atherosclerosis? • Extraanatomic bypass or angioplasty.
Total coronary revascularization with the internal thoracic arteries T graft • Follow-up: • Symptoms, stress test, thallium test. • Graft evaluation: • Duplex(supraclavicular fossa) :qualitative flow information in 95 % of cases. • Spiral CT scan : graft patency • sensitivity 85 %& specificity 100% • Angiography.