Download
1 / 27
270 likes | 413 Views
Marilyn Rose RT, RDMS. Nervous System. outline. Physiology Infections Meningitis Osteomyelitis of the skull Encephalitis Brain abscess Tumors Glioma Meningioma Acoustic neuroma Pituitary adenoma Craniopharyngioma Pineal tumors Chordoma Metastatic carcinoma.

E N D
Marilyn Rose RT, RDMS Nervous System
outline • Physiology • Infections • Meningitis • Osteomyelitis of the skull • Encephalitis • Brain abscess • Tumors • Glioma • Meningioma • Acoustic neuroma • Pituitary adenoma • Craniopharyngioma • Pineal tumors • Chordoma • Metastatic carcinoma
Outline contd • Trauma • Skull fracture • Epidural / subdural hematoma • Cerebral contusion • Intracerebral hematoma • Subarachnoid hemorrhage • Carotid artery injury • Facial fractures • Vascular disease • Stroke/ TIA • Intraparenchymal hemorrhage • Subarachnoid hemorrhage • MS • Epilepsy and convulsive disorders • Degenerative disease • Aging • Alzheimer's • Huntington’s dz • Parkinson’s dz • Cerebellar atrophy • Amyotrophic lateral sclerosis ( Lou Gehrig’s Dz) • Hydrocephalus • Sinusitis
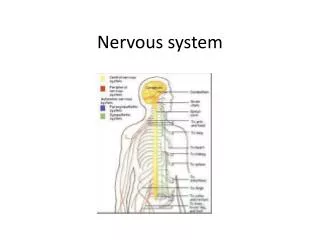
physiology • CNS - brain and spinal cord • PNS • 12 pairs of cranial nerves • 31 pairs of spinal nerves • Afferent (sensory) - Efferent (motor) • Somatic- striated skeletal muscles • Autonomic- smooth muscles of heart, glandular • Basic unit= neuron • Axon from the nerve body and one or more dendrites with a fatty covering called myelin sheath - > rate of transmission (deterioration= MS) • Involuntary reactions from CNS= reflex arc • Voluntary actions- reaction to stimulation • Synapse- impulses pass from one neuron to another • Cerebrum- two cerebral hemispheres • Gyri/sulci/ fissures • Cortex-outer (gray)cell body - inner(white)nerve fibers • CSF- formed by filtration of plasma from blood in choroid plexus of lat ventricles • Lateral ventricles- connect to 3rd by foramen of Monro • Fourth lies between the cerebellar hemispheres • 3rd and 4th are connected by aqueduct of Sylvius
Physiology contd • Cerebral cortex • Receive sensory information from all parts of the body- govern all motor activity • Visual impulses transmitted - posterior • Olfactory (smell) and auditory impulses - lateral • Higher functions like memory and creative thought • Corpus callosum- mass of white matter -connects two cerebral hemispheres • Between cerebrum/spinal cord= brain stem • Midbrain ( mesencephalon) • Pons • Medulla- vomit, cough, sneeze, hiccup, swallow • 12 cranial nerves • Centers for cardiac, vasomotor, respiratory
Physiology contd • Cerebellum- two lateral masses with the central vermis • Coordinates activities of groups of muscles to maintain equilibrium and posture • Diencephalon • Between cerebrum and midbrain • Located around 3rd ventricle • Thalamus- relay and processor of sensory information • Hypothalamus- link between mind and body- pleasure / reward • Release hormones • Regulate normal body temperature • Waking state
Physiology contd. • Spinal cord- w/in vertebral column • inner core -gray matter • surrounded by white matter tracts • conduct impulses up the cord • down the cord to spinal nerves • Brain/ spinal cord are protected by two layers: • Outer- cranial bone/ vertebral column • Inner- meninges • Pia mater- innermost layer adhering to outer brain and spinal cord • Dura mater- tough outermost covering- 3 extensions • falx cerebri- in longitudnal fissure- cerebral hemispheres • falx cerebelli – cerebellar hemispheres • tentorium cerebelli- covering over the cerebellum- occipital lobe/ cerebrum • Arachnoid membrane- delicate cobweb
infections • Meningitis • Acute inflammation of the pia and arachnoid • Middle ear, up resp tract or frontal sinus or by blood from lungs • Bacterial- (most common) • H influenzae in neonates/ peds • Meningococci/ pneumococci in adolescent/ adult • Viral- mumps, polio, herpes • Radiographic: • vascular congestion, edema • otherwise MRI and CT scans are normal • if infection extends…can cause diffuse brain swelling- • MRI and CT are useful in evaluating the complications..a/v vasculitis/ thrombosis, hydrocephalus or abscess. • A spinal tap is necessary to determine the cause • Osteomyelitis of the skull • Caused by direct extension • From paranasal sinus or scalp • Radiographic changes take 1-2 weeks to show • Radiographic: • Small multiple areas of lucency • Reactive sclerosis as bone tries to heal
Infections contd • Encephalitis • Viral inflammation • Mild headache/ fever- seizures and coma • 30% in children • Caused by herpes simplex= fatal • Radiographic: • Poor marginated- patchy temporal area • Mass effect is common- midline shift • Toxo- ring enhancement • Brain abscess • Chronic infection- middle ear, paranasal sinus- or systemic infection- pneumonia, bacterial endocarditis, osteomyelitis • Step most common • AIDS- toxo and cryptococcosis are common causes • Radiographic: • Area of abnormal density- poor defined borders • vascular edema • liquafaction • MRI is the best modality
Tumors • Intracranial Neoplasm -Manifest • seizure disorders • neurologic deficits • 50 % primary and 50% are mets • Radiographic: • Depend on location/ Site of mass effect • MRI is most sensitive for suspected tumors • Tumor extent and hydrocephalus • Brain stem and posterior fossa • Gliomas- most common primary malignant brain tumor • glial cells • Peak incidence in midlife- rare <30 yrs • Glioblastomas- mainly cerebral, malignant • Astrocytomas- 70% slow growing, infiltrative- pseudocyst • cerebrum, cerebellum, thalamus, optic chiasm and pons • Ependymomas- wall of 4th ventricle- children, lateral vents in adults • Medulloblastoma- rapid growing- disseminated in spinal fluid- subarachnoid • Oligodendrocytomas- slow growing arise in cerebrum- ca++ • Radiographic: • gliomas appear as masses of high signal intensity • single nonhomogeneous mass • glioblastomas have both increased and decreased density • Irregular ring of contrast enhancement
Tumors contd • Meningioma • Benign tumors of arachnoid • Attached to dura • Common sites- calvaria, olfactory groove, tuberculum sellae, spinal canal (25% of spine tumors) • Radiographic • Anatomic distortion • Isointense with brain tissue • Thin rim of low intensity, CSF cleft, vascular rim, ca++ w/in • Contrast enhances • Abut ting the dural surface • Acoustic neuroma • Slow growing benign tumor • Solitary or part of neurofibromatosis • Inner auditory canal- vestibular portion • Radiograph • Focal or generalized enlargement of the 8th cranial nerve • Erosion of the auditory canal • Large tumors can compress the 4th ventricle- hydrocephalus
Tumors • Pituitary adenoma • Anterior lobe- 10 % all intracranial tumors • Most nonsecreting chromophobe adenomas • Enlarge- adjoining secreting cells w/in sellaturcica are compressed leading to < secretion and < levels of growth hormone, gonadotropin,thyrotropic and ACTH hormones • Can distort optic chiasm • A hormone secreting pituitary tumor • hyperseceretion of growth hormone • gigantism prior to epeiphyses closure - pediatrics • acromegaly - adults • Excess secretion of adrenocorticotropic= • hypersecretion of steroid= Cushing’s disease • TSH= hyperthyroidism, • prolactin= galactorrhea-amenorrhea syndrome • Radiographic • Homogeneous and hyperdense to surrounding brain • Adjacent bone erosion • Compression of optic nerves, 3rd ventricle • MRI is the best modality
Tumors • Craniopharyngioma • Benign cystic and solid lesions • < 20 years of age • Arise anterior to sellaturcica from embryonic remnants • Depresses optic chiasm and extend into 3rd ventricle • Radiographic • Ca++ like eggshell on the periphery of a mixed cystic and solid lesion. • Hydrocephalus is Foramen of Monro is compressed • Pineal tumors • Germinomas and teratomas, rapid growing germ cell • Males < 25 yrs • Associated with precocious puberty • Radiographic • Sagittal MRI are ideal • Compress midbrain- lift up the splenium or the corpus callosum • Teratomas can have a mixed intensity- cystic and fat • Punctate ca++ is seen within the mass
Tumors • Chodoma • Arise from remnant of the notochord (embryonic neural tube)- or any part of the vertebral column or base of skull • Clivus and lumbosacral region most common • Locally invasive but not metastatic • Radiographic • Bulky mass- ill defined bone destruction or cortical expansion • Cloudlike (flocculent) ca++ can develop within a soft tissue mass • Metastatic carcinoma • Hematogenous spread • Most common metastasis is from the lung and breast • Melanoma, colon cancer , testicular and kidney tumors also cause brain mets • Radiographic • Singel or multiple masses of high signal intensity • Situated at the junction of gray and white matter
Trauma- skull • Skull fx • Linear- sharp lucent line on xray- irregular, jagged • Must distinguish from suture- which are serrated, bilateral and symmetrical • Diastaticfx- intersects a suture and courses along it • If fx involves: • vessel laceration= epidural hematoma • Sinus/ mastoid air cells- air is seen in ventricles • fragment of bone can be depressed into the cranial cavity- stellate or star shaped • Need tangential views to appreciate depth. • Basilar skull fx- air/ fluid level in sphenoid sinus • Complication of basal skull fx- CSF leak, meningitis and damage to facial nerve • PRESENSCE OR ABSENCE OF A SKULL FX DOES NOT CORRELATE WITH INTRACRANICAL ABNORMALITIES
Trauma- facial • Nasal bone (most common) • Range from simple-nondisplaced, to comminuted with depression of the septum • Best seen on R/L soft tissue lat projection • Blowout • Blow to the front of the orbit- thin orbital floor fx • Modified Water’s • Zygomatic arch • Blow from side of face- inward displacement of central fragments- outward displacement of zygomatic and temporal ends of arch • Jug handle view- submentovertex projection • Tripod • Fx to zygomatic arch and orbital floor- free floating zygoma • Mandible • Oblique views- angle is most common but bilateral fx are also common • Le Fort • Severe injury with separation and formation of large detached fragment- bilat and horizontal fx of the maxillae- type I,II or III
Trauma- epidural vs subdural • Epidural • Acute arterial bleed • Most common over parietotemporal convexity • Laceration • High pressure • Rapid mass effect • Acute neurologic symptoms • Radiographic • Biconvex, peripheral, high density • Midline shift to the opposite side • Subdural • Venous bleeding • Ruptured veins between dura and meninges • Low pressure • Chronic course- headache, agitation, confusion, drowsiness and gradual neurologic deficits • Radiographic • Peripheral zone of increased density follows surface of the brain in crescentic, mass effect with displacement of midline structures • Absence of midline shift can indicate bilateral subdural hematomas
Trauma-bleed • Cerebral contusion • Movement of the brain within the calvaria after blunt trauma to the skull • Patient looses consciousness- cannot remember • Radiographic • Low density edema, multiple small areas of hemorrhage • Frontal and anterior temporal regions most common • Post IV contrast will enhance for several weeks • Intracerebralhematoma • Shearing forces to intraparenchymal arteries • @ the junction of gray and white matter • Cause traumatic aneurysms to rupture • Radiographic • Well-circumscribed homogeneous, high density surrounded by low density edema- becomes isodense • Subarachnoid hemorrhage • Injury to surface veins, cerebral parenchyma or cortical arteries • Bleeding into ventricular system • Radiographic • Increased density within the basilar cistern, cerebral fissure and sulci • Identifying the falx on noncon CT is an indication of of subarachnoid blood
Trauma- bleed • Carotid artery injury • Extracerebralcarotid • injured from penetrating trauma- gunshot or stab • Trauma to internal carotid associated with 50% of traumatic fistulas • Radiographic • Angiography- demonstrate a laceration • dissection, thrombotic occlusion • Hyperextension- motor vehicle accident • intimal damage to carotid or vertebral- pseudoaneurysm • Traumatic arteriovenous fistulas arise between internal carotid and cavernous sinus Lt carotid dissection Traumatic aneurysm
Vascular disease • (1) Stroke • Sudden focal neurological deficit • Range from hemiplegia- coma to a trivial neurologic disorder • Neurologic defect depends on artery involved • Acute brain infarction- internal carotid artery • Symptoms- acute hemiparesis, dysarthria • Radiographic- rule out other causes for the symptoms • Rule out intracranial hemorrhage before using anticoagulants • Radiographic • Non con CT or MRI- best to evaluate for stroke • IV contrast is contraindicated- blood brain barrier - > edema and slower recovery • CT can be normal with a small infarct- large- will show a triangular shape hypodensity • Mass effect is maximal at 7-10 days • As the Infarct ages-brain tissue atrophies and adjacent sulci and ventricles enlarge • MRA is more sensitive to evaluate the edema and evolution
Vascular disease • (2) TIA • Manifest as focal neurological - resolve within 24 hours • May result from emboli – plaque • Temporary occlusion of cerebral vessels • Stenosis of an extracerebral artery- reduction in blood perfusion to the brain • 2/3 athrosclerotic strokes are preceded by TIA • Radiographic • Most common location of surgically treatable athroscleroticdz is carotid bifurcation in the neck • Asymptomatic bruit • Carotid duplex ultrasound is the preferred method to begin evaluation of the neck vessels. • Second evaluation is done by a MRA • May still need angiography or can rule it out with the US and MRA • Stenosis >60 % indicated advanced disease and requires surgical intervention • Anticoagulation therapy or endarterectomy
Vascular disease • (3) intraparenchymal hemorrhage • Principal cause- hypertensive vascular disease • Less common- rupture of Berry aneurysm or AVM • Significant mass effect • HTN hemorrhage most common in basal ganglia, white matter, thalamus, cerebral hemispheres and pons • Common complication is hemorrhage into ventricular system or subarachnoid space (subarachnoid hemorrhage) • Radiographic • MRI or non CON CT • Fresh hematoma- homogeneous dense round to oval shape • Hematoma- ventricular compression • considerably large- midline shift and brain herniation • Contrast enhancement develops around the periphery after 7-10 days • If pt has an aneurysm- it is important to locate the number of them • < 20 years of age- AVM is most common cause • On MRI a mass of vascular structures or CT an irregular tangle of vessels after contrast Subarachnoid- Berry rupture
Multiple Sclerosis (MS) • Most common demyelinating disorder • Recurrent attacks of focal neurologic deficits • Spinal cord, optic nerves ,white matter -brain • Peak incidence- 20-40 years- women • Multiple relapse and remission • Impairment of nerve conduction • degeneration of myelin sheaths- • Symptoms- • double vision, nystagmus(involuntary movement of eyeball in all directions), loss of balance and poor coordination, shaking tremor, muscular weakness, difficulty in speaking clearly and bladder dysfunction • Radiographic • MRI best modality • Scattered plaques of demyelination involve primarily • Periventricular white matter, cerebellum, brainstem and spinal cord • Optic nerve or chiasm- require contrast • CT during an acute episode and distinguish old plaque (non enhancing) from new active foci (enhancing) lesions.
Epilepsy/ Convulsive • Condition of brain impulses are temporarily disturbed • Spectrum of symptoms • loss of consciousness for a few seconds to violent seizures • Idiopathic- Can be the result of injury • trauma, depressed skull fx, birth trauma or infection • Mildest- petit mal • children- brief loss of consciousness and mild muscular twitching- disappear in adolescent • Grand mal- generalized convulsions- • pt falls to floor, hypersalivates and losses control of urine and feces • An approaching seizure- aura, ringing in ear, tingling in fingers or spots before the eyes.Radiographic • Wait until patient is clinically stable • MRI to evaluate for a brain tumor • AVM or hippocampal sclerosis- most common cause for seizure that do not respond to therapy. • Otherwise CT/ MRI are normal Eight patients of all epileptic symptoms were cured by the team during the study.
Degenerative Disease • Normal aging • Gradual loss of neurons- • enlargement of ventricular system and sulci • Alzheimer's • Presenile dementia- • diffuse form of progressive cerebral atrophy- • develop earlier than senile period • Huntington’s • Inherited- autosomal dominant- men • Early to middle adult- dementia • Choreiform movements- involuntary- rapid, jerky, continuous • Atrophy of caudate nucleus and putamen- focal dilation of frontal horns • Parkinson’s • Shaking palsy • Progressive- stooped posture, stiffness and slowness of movement • Basal ganglia • Enzyme defect resulting in inadequate production of neuronal transmitter dopamine (l-dopa) • Cerebellar atrophy • Inherited, degenerative or toxic effect of drugs as alcohol and phenytoin (Dilantin) • Lou Gehrig’s • Amyotrophic lateral sclerosis • Progressive – unknown cause • Atrophy and loss of motor nerve cells leading to extensive paralysis and death from respiratory weakness or aspiration pneumonia
Hydrocephalus • Dilation of the ventricular system • Increased intracranial pressure • Noncommunicating (obstructive) • Obstruction of CSF along the pathway • Enlarged lateral- normal 3rd- foramen of Monro • Enlarged lateral, 3rd- normal 4th-aquaduct of Sylvius • Enlarged system- Dandy Walker cyst at 4th vent • Communicating (nonobstructive)- more common • Generalized ventricular enlargement • Sulci normal or absent • Syndrome of gait ataxia, urinary incontinence, dementia are associated with ventricular dilation- with normal CSF pressure
Sinusitis • Paranasal sinuses • Maxillary, ethmoid, frontal, and sphenoid • Paired , air-filled cavities lined with mucous membrane • Size and shape vary in different age periods • Ethmoid- 6 yrs • Frontal- 10 yrs • Sphenoid- 2-3 and mature by adolescence • Viral infections cause upper respiratory obstruction with pain/ tender/ fever • Radiographic • Mucosal thickening • Water’s- patient erect- demonstrate air/ fluid levels • CT now modality of choice • MRI for complications such as mucocele, osteomyelitis and underlying intracranial dz