Download
1 / 20
230 likes | 296 Views
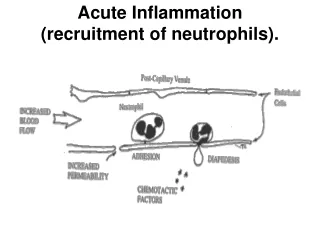
Possible outcomes of acute inflammation. Complete resolution Little tissue damage Capable of regeneration Scarring (fibrosis) In tissues unable to regenerate organized into fibrous tissue Abscess formation occurs with some bacterial or fungal infections Progression to chronic inflammation.

E N D
Possible outcomes of acute inflammation • Complete resolution • Little tissue damage • Capable of regeneration • Scarring (fibrosis) • In tissues unable to regenerate • organized into fibrous tissue • Abscess formation occurs with some bacterial or fungal infections • Progression to chronicinflammation
CHRONIC INFLAMMATION The processes of inflammation & healing (granulation tissue) proceed side by side
Chronic inflammationThe processes of inflammation & healing proceed side by side • Lymphocyte, macrophage, plasma cell (mononuclear cell) infiltration • Tissue destruction by inflammatory cells • Attempts at repair with fibrosis & angiogenesis (new vessel formation)
Chronic Inflammation • Long term (≥≥ days). • Characterized by the presence of macrophages, lymphocytes & plasma cells. • Accompanied by the proliferation of blood vessels & connective tissue (granulation tissue).
CHRONIC INFLAMMATION • may develop in the course of • Persistent / recurrent infection • or progressive acute inflammation • or low grade irritants that fail to elicit an acute response
Chronic inflammation • Persistent injury or infection (ulcer, TB) • Prolonged toxic agent exposure (silica) • Autoimmune disease states (RA, SLE)
Chronic InflammationThe Players • Macrophages process & deliver antigen to immunocompetent cells — mediate immune reactions. • Lymphocytes and plasma cells are involved in the immune reactions
The Players (mononuclear phagocyte system) • Macrophages • Scattered all over • Circulate as monocytes and reach site of injury within 24 – 48 hrs and transform • Become activated by T cell-derived cytokines, endotoxins, & other products of inflammation
The Players • T & B lymphocytes • Antigen-activated (via macrophages and dendritic cells) • Release macrophage-activating cytokines • in turn, macrophages release lymphocyte-activating cytokines • Plasma cells • Terminally differentiated B cells • Produce antibodies
The Players • Eosinophils • Found especially at sites of parasitic infection, or at allergic (IgE-mediated) sites
Types • NONSPECIFIC CHRONIC INFLAMAMTION- Diffuse accumulation of macrophages and lymphocytes at injury site Macrophages from 3 sources: 1) recruitment 2) local proliferation 3) prolonged survival
B. GRANULOMATOUS INFLAMMATION Granuloma formation –collection of modified macrophages Resemble squamous cells, therefore called “epithelioid” • surrounded by lymphocytes
Granulomatous Inflammation • Clusters of T cell-activated macrophages, which engulf and surround indigestible material (mycobacteria, foreign bodies) • Depostion of antigenic material, type IV hypersensitivity reaction
CD IFNg IL-12 TNFb IL-2 CD4+ Th1 cytokines IL-12 Proliferation Granuloma Formation IL-1, TNFa, IFNg, IL-12, GM-CSF, MIP-1a MF IL-8, IL-15, IL-16, RANTES TGF-b PDGF IGF-1 Fibrosis GRANULOMA FORMATION
In the usual hematoxylin and eosin–stained tissue sections, • the epithelioid cells have a pale pink granular cytoplasm with indistinct cell boundaries, often appearing to merge into one another. • The nucleus is oval or elongate and slipper/shoe/footprint shaped (folding of the nuclear membrane)
epithelioid cells fuse to form giant cells. • These giant cells may attain diameters of 40 to 50 μm. • containing 20 or more small nuclei arranged either peripherally (U /semicircle/garland/horse-shoe shape) - Langhans-type giant cell or haphazardly - foreign body–type giant cell
Foreign Body Reaction • Indicated by the presence of multinucleated foreign body giant cells and the components of granulation tissue (macrophages, fibroblasts, and capillaries) • The biomaterial will often determine the composition of the foreign body response