Download
1 / 27
300 likes | 767 Views
Acute inflammation. Formation of acute inflammatory exudate From: Stevens A. J Lowe J. Pathology. Mosby 1995. Fig.5.1. Chemical mediators acting on nearby blood vessels from inflammatory focus. Fig.5.2. Vasodilation and increased permiability. Fig.5.3. Neutrophils margination and emigration.

E N D
Formation of acute inflammatory exudateFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.1. Chemical mediators acting on nearby blood vessels from inflammatory focus
Fig.5.2. Vasodilation and increased permiability
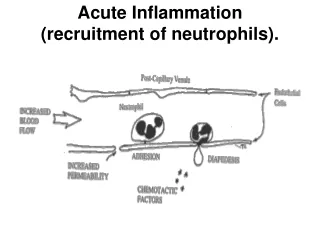
Fig.5.3. Neutrophils margination and emigration
Neutrophil margination, emigration and emigration in acute inflammationFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.4. Neutrophil margination, emigration and emigration in acute inflammation
Neutrophil margination and emigration in acute inflammation Fig.5.5.
Neutrophil margination, emigration and emigration in acute inflammation Fig.5.6.
Neutropil phagocytosis From: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.7.
Mechanisms involved in inflammation-From: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.8.
Acute serous inflammationFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Acute amigdalitis Fig.5.9.
Herpetic inflammation Fig.5.10.
Serous alveolitisFrom cases of the Pathology Department U.M.F. “Gr. T. Popa” Iasi Fig.5.11.
Fig.5.12. Serous alveolitis: (1) Alveolar walls (congestion of parieto-alveolar capillaries); (2) Alveolar lumen: serous exudate.
Fibrinous inflammationFrom cases of the Pathology Department U.M.F. “Gr. T. Popa” Iasi Mallory staining Fig.5.13.
Mallory staining Fig.5.14. Fibrinous alveolitis: (1) alveolar walls (congestion of parieto-alveolar capillaries); (2) alveolar lumen: fibrinous exudate.
Fibrinous pericarditisFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.15. Fibrinous deposits on parietal pericardium
From cases of the Pathology Department U.M.F. “Gr. T. Popa” Iasi Fibrinous pericarditis: (1) Epicardium is covered by fibrinous exudate forming intense eosinophilic fibrin network; (2) Epicardium with vascular congestion and neutrophils. Fig.5.16.
Acute purulent inflammation Fig.5.17. Pus smear (May Grunwald Giemsa) Purulent exudate (pus) iscomposed of:neutrophiles; macrophages; eritrocytes; necrotic debris; fibrin; bacteria.
Fig.5.18. Pus smear (MGG) From cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi
Acute diffuse purulent inflammationFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Purulent leptomeningitis Fig.5.19.
Purulent leptomeningitis: (1) meninges is diffusely thickened by purulent exudate and vascular congestion. (2) - congested vessels(leukocyte margination and diapedesis). HE staining Fig.5.20. From cases of the Pathology Department - U.M.F. “Gr. T. Popa” Iasi
Fig.5.21. HE staining Vascular congestion and leukocyte diapedesis
Fig.5.22. HE staining Leukocyte margination and diapedesis From cases of the Pathology Department - U.M.F. “Gr. T. Popa
Acute localised purulent inflammationLung acute and chronic abscessesFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.23.
PulmonaryabscessFrom: Stevens A. J Lowe J. Pathology. Mosby 1995 Fig.5.24. Pulmonary abscess: (1) the cavity: contains a suppurative material and air content (in case of communication with air conducts); (2) wall: (a) acute abscess – the wall has irregular borders reprezented by suppurative necrotic lung parenchyma; (b) chronic abscess - the wall is a pyogenic membrane that becomes fibrotic by connective organization.
Localised purulentinflammation(abscess) Fig.5.25. From cases of the Pathology Department U.M.F. “Gr. T. Popa” Iasi HE staining • Abscess: • Localized purulent Inflammation; • Types • acute / recent • chronic Recent cerebral abscess • center: • purulent exudate; • periphery: • fibrin wall.
Cronic hepatic abscess • central cavity contains • purulent exudate; • peripheral wall - pyogenic membrane • external layer • connective-vascular tissue of neoformation • internal layer • fibrin network • neutrophils Fig.5.26. From cases of the Pathology Department U.M.F. “Gr. T. Popa” Iasi