Download
1 / 32
360 likes | 652 Views
HEPATIC DISORDERS. NUR – 224. LEARNING OUTCOMES. Explain liver function tests. Relate jaundice, portal hypertension, ascites, varices, nutritional deficiencies to the pathophysiology of the liver.

E N D
HEPATIC DISORDERS NUR – 224
LEARNING OUTCOMES • Explain liver function tests. • Relate jaundice, portal hypertension, ascites, varices, nutritional deficiencies to the pathophysiology of the liver. • Use the nursing process as the framework for the care of the patient with cirrhosis of the liver
LIVER • Largest gland in the body /complex organ • Located on the right side of the abdomen – anterior to the stomach • Highly vascular organ • Circulation of blood to the liver is of major importance. • Multiple metabolic and regulatory functions
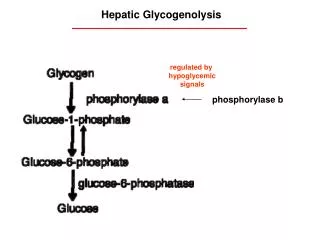
ESSENTIAL FUNCTIONS • Secretes bile • Stores fat-soluble vitamins (A, B,D, and several B- complex vitamins) • Metabolizes medication – barbiturates, opioids, sedatives, amphetamines, anesthetics • Active in fat/protein metabolism. • Releases glucose during times of hypoglycemia • Takes up glucose during times of hyperglycemia and stores it as glycogen or converts it to fat • Store iron as ferritin – which is released as needed for the production of RBC’s • Converts ammonia to urea
DIAGNOSTIC STUDIES • Liver Function test • Liver biopsy
LIVER BIOPSY • Performed to r/o metastatic cancer, detect cyst, or cirrhosis of the liver • Considered minor surgery • Results of coagulation test – PTT, PT, platelet count • Signed consent • Withhold any anticoagulants, ibuprofen, ASA – for a week prior to the procedure • Food/fluids withheld 4-6 hours before the procedure • Void prior to the procedure
LIVER BIOPSY Post procedure • Client lies on the right side, immobile for several hours • Avoid coughing and straining • Monitor vital signs • Avoid heavy lifting, strenuous activity for 1 week
COMMON MANIFESTATIONS OF LIVER DISORDERS • Jaundice • Ascites • Portal hypertension • Esophageal varices • Hepatic encephalopathy
Jaundice • Disrupted metabolism/excretion of bilirubin accumulates in the tissues --jaundice • yellow staining of the body tissues • First noticeable in the sclera of the eyes, then the skin • Concentration of bilirubin in the blood is abnormally increased Types • Hemolytic • Hepatocellular • Obstructive
Portal Hypertension • Impaired/obstruction blood flow through the liver increases pressure in the portal venous system drains into the GI system, spleen and surface veins of the abdomen. • Leads to: ascites esophageal varices
Ascites • Accumulation of serous fluid in the peritoneal/abdominal cavity • Contributing factors portal hypertension, increase flow of hepatic lymph system, and hyperaldosteronism. • Common manifestation of cirrhosis • Large amounts albumin-rich fluid fills the peritoneal cavity (12-15 L)
Manifestations of Ascites • Abdominal distention • Rapid weight gain • Signs of dehydration • Decrease in urine output • Hypokalemia
Treatment of Ascites • Sodium restriction • Diuretics • Fluid removal - paracentesis • Bedrest • Shunt procedures – transjugular intrahepatic portosystemic shunt (TIPS)
Esophageal Varices • Develop on a majority of patients with cirrhosis • Dilated, tortuous vessels that develop at the lower end of the esophagus • Enlarged and swollen as a result portal hypertension • Are responsible for approx 80% of variceal hemorrhages
Bleeding Esophageal Varices • Life threatening and led to shock • Varices rupture and bleed in response to ulceration and irritation • Contributing factors • Clinical manifestations – hematemesis, melena, hx of alcohol abuse, s/s of shock may be present • Diagnostic findings - endoscopy
Treatment of Bleeding Varices • Treatment of shock • Oxygen • IV fluids with electrolytes • Vasopressin, somatostatin, octreotide • Beta-blocker agents • Balloon tamponade • Endoscopic therapies
Nursing Management • Monitor patient condition physical, emotional and cognitive status • Assess nutritional and neurologic status – increase ammonia levels drowsiness, confusion • Monitor tube care and GI suction • Oral care • Quiet calm environment
Hepatic Encephalopathy • Impaired consciousness and mental status accumulation of toxic waste products in the blood blood bypasses the congested liver • Ammonia is considered the major etiologic factor in the development of encephalopathy. • Life threatening complication of liver disease • Associated with portal hypertension and the shunting of blood from the portal venous into the systemic circulation
Hepatic Encephalopathy • Onset insidious • Clinical manifestations early symptoms – minor mental changes/motor disturbances late symptoms – incomprehensible speech, marked confusion • Asterixis • Apraxia • Fetor hepaticus
Management Hepatic Encephalopathy • Eliminate precipitating factors • Administer lactulose as ordered • Assess neurologic status frequently • Monitor mental status • Administer antibiotics • Discontinue sedatives, analgesics and tranquilizers • Prevent development of respiratory complications
Cirrhosis • Chronic progressive disease • Normal liver tissue is replaced by fibrous liver tissue that disrupts the structure and function of the liver • 12th leading cause of death in the US • Death rate is twice as high in men than women • Native American men have the highest incidence and mortality rate from cirrhosis
Pathophysiology • Functional tissue is destroyed and replaced by fibrous tissue. • Hepatocytes and liver lobules are destroyed , metabolic function of the liver is lost. • Fibrous connective tissue forms constructive bands that disrupt blood and bile flow within the liver lobules • Blood no longer flows freely through the liver to the IVC • Restricted blood flow portal hypertension, increased pressure in the portal system
Cirrhosis Types • alcoholic – end result of alcoholic liver disease • postnecrotic – results from chronic hepatitis B or C, NAFLD • biliary – retained bile damages and destroys liver cells
Clinical Manifestations • Onset insidious Early signs • Dull aching pain – epigastric area/RUQ • Weight loss, weakness, • Bowel function disrupted – diarrhea/constipation Late signs Impaired metabolism bleeding, ascites, jaundice, neurological changes, splenomeagly GI varices, edema, vitamin deficiency, and anemia
Assessment & Diagnostic Findings • Liver function tests • Coagulation studies • Serum electrolytes • Serum ammonia levels • CBC with platelets • Abdominal ultra sound • Liver biopsy
Collaborative Care • Medications • Fluid Management/Nutrition
Nursing Process • Excess Fluid Volume • Risk for Bleeding • Impaired Skin Integrity • Risk for Acute Confusion
Practice Alert • Monitor for signs of impaired renal function oliguria, central edema and increase in serum Crt/BUN. • Closely monitor patient who have GI bleeding assess for signs of hepatic encephalopathy. • Monitor the respiratory status of the patient with a Blakemore/Minnesota tube.