1 / 5
50 likes | 174 Views
Definition and Grading of Hepatic <br>Encephalopathy, diagnosis and treatment, coma scale

E N D
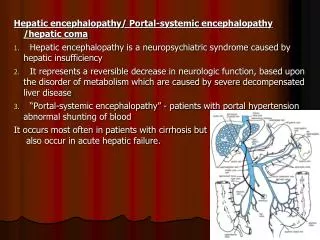
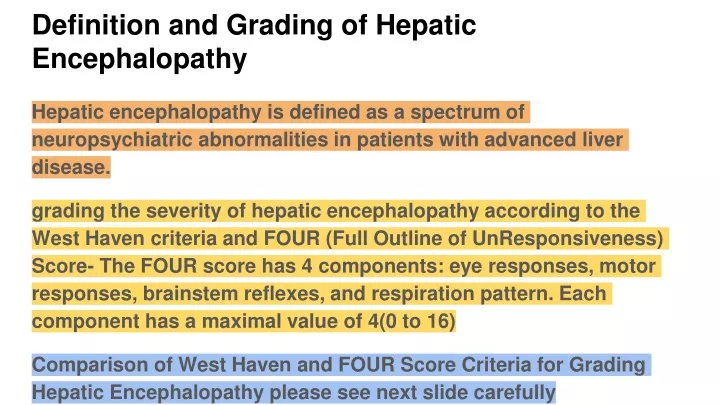
Definition and Grading of Hepatic Encephalopathy Hepatic encephalopathy is defined as a spectrum of neuropsychiatric abnormalities in patients with advanced liver disease. grading the severity of hepatic encephalopathy according to the West Haven criteria and FOUR (Full Outline of UnResponsiveness) Score- The FOUR score has 4 components: eye responses, motor responses, brainstem reflexes, and respiration pattern. Each component has a maximal value of 4(0 to 16) Comparison of West Haven and FOUR Score Criteria for Grading Hepatic Encephalopathy please see next slide carefully
Wijdicks EF. N Engl J Med 2016;375:1660-1670. Mechanisms Underlying Hepatic Encephalopathy and Brain Edema.
Diagnosis Blood serum ammonia level (Hyperammonemia results in neuronal dysfunction, leading to hepatic encephalopathy and may lead to Brain edema(acute liver failure) CT scan- Disappearance of sylvian fissures and sulci characterizes early brain edema MRI EEG (Triphasic-wave patterns appear in grade 2 or 3 hepatic encephalopathy but disappear in the comatose state) electrolyte panel (Sodium, calcium, potassium, chloride, phosphate)
Treatment First line Rx:- Guidelines recommend lactulose at a dose of 25 ml twice daily (These nonabsorbable disaccharides have laxative effects and change the gut microbiome to non–urase-producing bacteria, reducing intestinal ammonia production) Intravenous l-ornithine–l-aspartate:-( lowers ammonia levels by providing an alternative substrate for the urea cycle; its use is considered in patients who do not have a response to lactulose) rifaximin (550 mg twice a day),For recurrent hepatic encephalopathy in patients with cirrhosis Probiotics (yogurts with lactobacillus or saccharomyces) SECOND-LINE TREATMENTS portosystemic shunts, liver transplantation (in End-stage liver disease)