Download
1 / 41
410 likes | 757 Views
Plasticity of the Immature Brain: Sensory Deprivation, Focal Lesions. Shani Hagler Isabelle Rapin Child Neurology: September 25, 2013 No conflict of interest. Brain Plasticity. The structure of the brain is a function of the genetic programs that orchestrate its development and

E N D
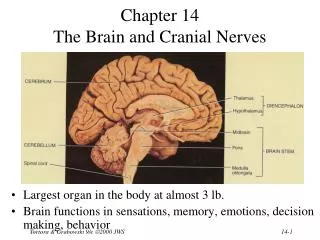
Plasticity of the Immature Brain:Sensory Deprivation, Focal Lesions Shani Hagler Isabelle Rapin Child Neurology: September 25, 2013 No conflict of interest
Brain Plasticity The structure of the brain is a function of • the genetic programs that orchestrate its development and • inputs from the environment
Environmental effect on development of cortical neurons in fish: Brought up alone Brought up with others Cover of Science!
Brain Plasticity In humans and animals damage or sensory deprivation → • structural alteration (limited) of subcortical relays and sensory cortex • potential for (partial) functional recovery / substitution
Brain Plasticity Lack of major sensory input (deafness, blindness, limb amputation, etc.) → major reorganization of sensory cortex, with spared modalities occupying (partially) deafferented sensory areas
Variables that affect brain reorganization • Age at sensory deprivation • Completeness of the sensory loss • Interval since sensory loss • Stimulation following the sensory loss
Unilaterally Deafened Animals: Subcortical Plasticity • More immature animals →greater effect • Sound deprivation, cochlear destruction →structural reorganization of brainstem nuclei, competitive innervation • Decreased number, smaller neurons • Dendritic atrophy e.g., Webster, Clopton, Parks, Rubel
Human: Subcortical Plasticity • Down infant(middle ear effusion) → • ventral cochlear nuclei smaller; fewer neurons • Cockayne syndrome(cochlear degeneration) → • ventral cochlear nucleus, medial olive, inferior colliculus: neurons small • medial geniculate, Heschl gyrus: neurons normal ! Gandolfi, 1981, 1993
Plasticity: Differences in Early Sound Exposure in Animals → • Decrease affects sound localization and visual/auditory maps in tectum • Patterned sound exposure affects sound selectivity of collicular neurons in rats, mice • Selective cochlear lesions change tonotopic map in auditory cortex in cats • Discrimination training changes tonotopic map in auditory cortex in owls • Deafness increase visual responses in auditory cortex in cats
Plasticity: Early Speech Sound Exposure in Humans • Neonate: makes many speech sound discriminations • 1 year old:loss of irrelevant, honing of relevant speech sound discriminations • Toddler/preschooler: learn new language accent-free • Older child/adult: accented new language; do not hear irrelevant contrasts (e.g. L/R)
Bilateral Congenital Vestibular Dysfunction: Effect on Sitting and Walking (N=22) • No nystagmus or vertigo • May have delayed head control, hypotonia • Age at sitting: 8 months ( 6 – 24) • Age at walking: 16.5 months (10 – 48) • Danger: swimming under water • Rapin 1974
Brain differences in early blindness Normally - 1/3 of cortex involved in visual processing Blinded animal studies: new projections from inferior colliculus (auditory) to lateral geniculate nucleus (normally visual) Anatomy: - Gray&white matter atrophy of visual networks - Increase in cortical thickness in cuneus (decreased pruning?) Metabolism: - 15% ↑ glucose metabolism in striate and extrastriate cortex Kupers et al, 2011
Brain imaging in congenital/early blindness A. Gray matter - red, white matter - blue B. Increased cortical thickness of cuneus C. Increased glucose metabolism Kupers et al. 2011
Cross-modal plasticity Kupers et al 2011 Ptito et al 2008 Cohen et al 1999 Frasnelli et al 2011 Occipital cortex (OC) - shift from processing visual other sensory modalities ? explains extraordinary auditory & tactile abilities in the blind TACTLE: - ↑ tactile acuity - Braille activates OC only in congenital/early onset blindness - TMS disrupting occipital lobe errors in Braille & paresthesias in fingers - TDU (computer game) training for one week blind activated visual cortex AUDITORY: - 1/2 EOB: ↑ localization mono-aural sound - activates specific OC areas SPACIAL PERCEPTION: - CB unaffected by hand crossing in determining order of hand touched
Crossmodal plasticity in early blind OLFACTION - ↑ odor identification - odor detection →↑ blood oxygenation level- dependent (BOLD) responses in primary & higher order olfactory & occipital cortices HIGHER CORTICAL FUNCTION - repetition priming (-rTMS) over to visual cortex → slows Braille reading Kupers et al 2011
Brain consequence of sensory deprivation Cortical reorganization hypothesis - cross-modal brain responses = formation of new pathways in the sensory-deprived brain vs. Unmasking hypothesis - loss of a sensory input → unmasking and strengthening of preexisting neuronal connections Kupers et al 2011
Plasticity in focal early lesions in visual pathway Less clearly correlated field cuts with early than late focal lesions Infant with perinatal stroke of L optic radiations - at 3 months: visual cortical activation only of unaffected side - at 20 months: activation of visual cortex on affected side reorganization of thalamo-cortical pathway Early visual field defecit - less ↓ in environmental navigation - in cats: entire visual cortex removed visual orientation unaffected due to reorganization of subcortical to extrastriatal visual pathways Seghier et al., 2004
Early lesions in central visual pathway in cat Damage Rt striate cortex: Damage Lt optic radiation • LEFT--potential by-pass of lesion potential full recovery of conscious vision. • RIGHT-- no full recovery of conscious vision. Expanded collicular -- extrastriate cortex ~ normal visual exploration & navigation • Cionni et al 2011
Corticospinal Tract Development Reaches cervical cord by 24 wks Begins myelination by 40 weeks Newborn: both ipsi- and contralateral corticospinal innervation of spinal motor neuron pools By 2yrs - Rapid differential development of the ipsilateral and contralateral tracts. Dominance of the contralateral (crossed) tract In hemiplegia: ipsilateral dominance progressively detrimental competes with residual contralateral tract JA Eyre et al., 2007
Sensorimotor Reorganization in CP* Motor: both ipsi- and contralesional cortical reorganization Somatosensory: predominantly ipsilesional reorganization motor + sensory lesion: interhemispheric dissociation of motor/sensory functions Motor cortex lesion – total loss of crossed tract rare - activity-dependent competition for ipsi- vs. contralesional access to spinal motor neuron pool (TMS & EMG) - role of somatosensory feedback from affected limb *pattern depends on timing, size, & location of lesion. Guzzella et al. 2007
Main types of sensorimotor reorganization in lateralized damage Cionni et al. 2011
CP & Hand Function Finger dexterity: correlation atrophy of thalamo-cortical > than cortico-spinal tract Contralateral slower than ipsilateral hand Bimanual: both slow “ : contralateral better than when unimanual Rose et al., 2011 Steenbergen et al., 2008
Hemiparetic CP in Perspective Dynamic motor deficit Immature cortico-spinal hemi not present beforeof 6 mos Worsening hemi: competition of uncrossed and crossed cortico-spinal tracts tract for spinal motor neurons Very early lesion: uncrossed tract may compensate Importance of sensory deficit for prognosis If sensory & motor reorginization in different hemispheres severity of deficits poorly coordinated Neglect: Lt lesion ± mild bilateral Rt lesion ± ↓attention, ↓ spacial skills Katz et al 1998
Language in the brain:distributed network • Language processing is bi-hemispheric: • Lt >> Rt: phonology, syntax, semantics • Rt >> Lt: prosody, pragmatics • Both (L >> R): lexicon • Lt. superior temporal: phonologic decoding • Lt. inferior frontal: encoding phonology/syntax • Suprasylvian temporo-parietal: lexical processing • Cerebellum: encoding automaticity etc. • Etc.
Language in early lateralized brain lesion • Language will develop whether lesion in the Rt or Lt hemisphere (plasticity) • Location of lesion does not predict type of language deficit !! • Language is delayed, but catches up by school age • Price to pay for plasticity: visuo-spatial deficits likely E. Bates et al.
Aphasia Cause: early focal lesion Language delayed Lesion location: not predictive of type ! articulation: OK Prognosis: ~ good reading ± OK often ↓ visual/spatial skills CT/MRI: informative Developmental Cause: ~ genetic Language delayed Several subtypes: most receptive/expressive, others expressive, fluent Prognosis: variable reading ~ impaired often: + other dev. disorder CT/MRI: ~ useless Early acquired aphasia vs. developmental language disorder
Acquired aphasia in toddlers/older children • Parallel the aphasia syndromes of adults • Recovery of language tends to be better than in adults but is by no means necessarily complete • Sequelae: depend on size/location of lesion • Sequelae: almost invariably reading/ academic problems ±cognitive deficits
Cortical Calculation Networks Dehaene, 2001
Calculation: Relevant Cortical Circuitry • Occipito-parietal (dorsal, “where”) visual stream intraparietal sulcus L > R • Occipito-temporal (ventral, “what”) visual stream fusiform gyrus • Lateral prefrontal cortex • Working memory • Attention • Executive skills
Dyscalculia Difficulty acquiring basic arithmetic skills Detected later than dyslexia Requirements: adequate language skills visuo-spatial skills memory, working (& long-term) executive skills, including attention
Children with dyscalculia Control children Kucian et al. 2006
Gerstmann syndrome (1920s) • In acquired Lt ~ angular gyrus lesion • R-L confusion • Finger agnosia • Dyscalculia • Dysgraphia • Developmental Gerstmann syndrome (Kinsbourne & Warrington 1963) • All of the above • Constructional dyspraxia
Roots of American lower SEM than Asians: School hours/week on language vs. math Stevenson et al., Science 1986 Japan Taiwan U.S.
Effect of Practice on the Brain • Violinists: ↑ cortical finger representation • Musicians vs non-musicians: altered hemispheric dominance for music • Wine tasters: much enhanced smell discrimintion • Dancers, athletes: enhanced cerebellar activation
Remediation • Training / education is the most powerful tool we have to alter / improve brain structure and function • But… brain plasticity is limited by • severity of pathology • location of pathology • age at time of insult • adequacy of the intervention!
Cochlear Implant • Requirement: viable neurons in spiral ganglion • Early in prelingual deafness: activates the central auditory pathway → quite effective • Late in prelingual deafness: activates primary but not secondary auditory cortex → more limited effectiveness • In previously hearing person→ effective • In all cases: requires intensive and prolonged training