Download
1 / 12
120 likes | 321 Views
GUSTO-IV AMI. G lobal U se of S trategies T o Open O ccluded Coronary Arteries in AMI. Why Abciximab and Reteplase. Preclinical and pilot clinical studies suggest that the combination of a IIb/IIIa inhibitor and a thrombolytic may:. Accelerate reperfusion Prevent reocclusion

E N D
GUSTO-IV AMI G lobalU se ofS trategiesT o OpenO ccluded Coronary Arteries in AMI
Why Abciximab and Reteplase Preclinical and pilot clinical studies suggest that the combination of a IIb/IIIa inhibitor and a thrombolytic may: • Accelerate reperfusion • Prevent reocclusion • Improve clinical outcome • Facilitate PCI • Protect the microcirculation and improve the microcirculatory flow
Rationale • The primary hypothesis to be tested is that Abciximab added to reduced dose Reteplase will improve clinical outcomes with equal or superior safety compared to conventional thrombolysis with Reteplase alone.
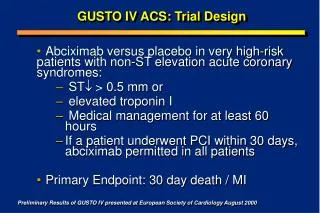
Study Objective • The primary objective of this study is to compare the effects of Abciximab (bolus + infusion) in combination with Reteplase (5 U + 5 U double bolus) and low-dose weight adjusted heparin (treatment), versus 10 U +10 U double bolus Reteplase with standard heparin (control) on the primary endpoint of all-cause mortality through 30 days.
Trial Design • Phase III • Multicenter, Multinational • Randomized • Open label • Approximately 800 sites • Approximately 16,600 patients
Trial Protocol (n = 16,600) ST , lytic eligible, < 6 hr ASA No Abciximab Abciximab* 2 x 10 U bolus (30’) Reteplase 2 x 5 U bolus (30’) Reteplase Standard Heparin: 5,000 U bolus followed by either 800 U/hr (pts < 80 kg) or 1,000 U/hr (pts > 80 kg) infusion Low Dose Heparin: 60 U/kg bolus followed by a 7 U/kg/hr infusion 1º endpoint: mortality at 30 days 2º endpoint: clinical and safety events at 30 days * 0.25 mg/kg bolus followed by 0.125 g/kg/min infusion for 12 hours
Major Inclusion Criteria • At least 18 years of age • Prolonged (> 30 minutes), continuous, ischemic pain with onset within 6 hours prior to randomization • ECG changes • > 2 mm ST-segment elevation in 2 or more contiguous leads • > 1 mm ST-segment elevation in 2 or more limb leads • Written informed consent
Major Exclusion Criteria • Planned primary percutaneous intervention • Active internal bleeding or history of hemorrhagic diathesis • Major surgery or serious trauma within the previous 6 weeks • History of cerebrovascular accident within the previous 2 years • Administration of oral anticoagulants within the previous 7 days
Laboratory Procedures • Baseline (within 6 hours prior to randomization) • Hemoglobin • Hematocrit • Platelet count • aPTT, PT or INR • Baseline (within 2 hours prior to randomization) • CK-MB (or Total CK if CK-MB not available) • 12-lead ECG • Post Procedure • ECG (hospital discharge or day 7; prior to transfer; or 12-24 hrs post revascularization procedure)
Efficacy and Safety Endpoints • All cause mortality at 30 days • Non-fatal disabling stroke through discharge or day 7 post-randomization (whichever is earlier) • All cause mortality through 1 year • Incidence of hemorrhagic stokes (including hemorrhagic conversion) through discharge or day 7 post-randomization (whichever is earlier)