Download
1 / 21
250 likes | 520 Views
Genetic Diseases. Lecture 51 Thursday, May 3, 2007 Ref. Basic Pathology Chapter 7. Ocular Genetics Review Article. Ocular Genetics: Current understanding. Ian M. MacDonald, Mai Tran, and Maria A. Musarella. Survey of Ophthalmology, 40 (2):159-196, 2004

E N D
Genetic Diseases Lecture 51 Thursday, May 3, 2007 Ref. Basic Pathology Chapter 7
Ocular Genetics Review Article • Ocular Genetics: Current understanding. Ian M. MacDonald, Mai Tran, and Maria A. Musarella. Survey of Ophthalmology, 40 (2):159-196, 2004 • Example: There are 11 publications identifying loci of genes associated with glaucoma. Three proteins have been identified: optineurin found in normal tension glaucoma, myocilin found in POAG, aggressive, and a cytochrome P450 CYP1B1 in primary congenital glaucoma. • In another study of 152 families, myocilin was an uncommon cause of POAG.
Genetics, Genomics & Proteomics • Genetics: The study of a single or a few genes and their phenotypes. • Genomics: The study of all the genes in the genome and their interactions. • Proteomics: The effort to identify and characterize all the proteins encoded in an organism’s genome including their post translational modifications.
Results of the human genome project • 30,000 genes • But > 100,000 proteins due to alternative splicing and other modifications • < 2% of genome codes for proteins • Any 2 individuals share 99.9% of DNA sequence
Congenital or hereditary • Congenital = present at birth • Not necessarily genetic; some disorders are caused by toxins, infection, hypoxia, etc. • Hereditary = transmitted from parents in gametes, therefore genetic • Not necessarily congenital, e.g. Huntington disease expression begins in middle age. • Familial
Types of mutations • Mutation- a permanent change in DNA • Point mutation- substitution of a single nucleotide • Silent • Missense (protein will have a different amino acid) • some substitutions make not difference • Nonsense (protein cannot be translated) • Additions/ deletions • If ≠ 3 nucleotides, frameshift occurs. • Frameshift often results in loss of that protein or a nonfunctional protein. • Frameshift may still make a functional protein • Example: O allele instead of A allele in blood types
Types of mutations cont’d • Trinucleotide repeats • Include G and C • Dynamic (# of repeats increases during gametogenesis) • Example: fragile X syndrome has 250-4000 repeats of CGG in FMR1 gene • Mutations involving large sequences of DNA • Translocations • Inversions
Rearrangements of chromosomes resulting in aberrations BP 7-17
4 Categories of genetic diseases • Mutant gene with large effect (Mendelian) • Also called single gene or monogenic disorder • Multifactorial and polygenic • Polygenic-more than one gene determines a trait • Many factors both genetic and environmental • Probably most common type of genetic disease • Chromosomal aberrations • Karyotype for diagnosis • Non-classical • Triplet repeat mutations • Mitochondrial DNA • Genomic imprinting -epigenetic phenomenon
Pleiotropy and heterogeneity • Pleiotropy- a mutation causes many phenotypic effects • Example: Marfan disease- mutation in fibrillin affects eye, skeleton, cardiovascular system • Genetic heterogeneity- mutations at several different loci produce the same trait • Example: retinitis pigmentosa ~30 loci
Mendelian disorders • See Table 7-1 for prevalence • Relatively common--familial hypercholesterolemia (1 in 500) • Transmission Patterns: • Autosomal dominant • Autosomal recessive • X-linked • Co-dominance-both alleles are expressed • Normal for MHC and blood group antigens • In an autosomal dominant disorder, 50% reduction in normal product gives abnormal phenotype
Familial hypercholesterolemia • Caused by a mutation in the gene for LDL receptor • Relatively common (1 in 500 are heterozygotes) • LDL receptor is critical for cholesterol metabolism; lack causes reduced catabolism and excessive biosynthesis • Autosomal dominant • Heterozygotes have ~2-3 fold elevation of serum cholesterol • Homozygotes have >5 fold increase in cholesterol levels.
Autosomal dominant disorders • Usually inherited from parent but can be new mutation • age when disease develops and severity of disease • Phenotype can be modified by: • Reduced penetrance • inherit the gene but have normal phenotype • Variable expressivity • The gene is expressed in everyone who inherits it, but the gene is expressed differently. • E.g. Neurofibromatosis Type 1 ranges from brownish spots on the skin to multiple tumors.
Autosomal recessive disorders • Usually expression is more uniform than dominant disorders. • Usually complete penetrance. • Often involve enzyme deficiency. • Heterozygotes are normal with 50% of enzyme. • Mechanism may be due to toxicity of intermediates . • Often have early onset. • Examples: cystic fibrosis, lysosomal storage diseases, sickle cell anemia, glycogen storage diseases.
X-linked disorders • Usually X-linked disorders are recessive. • Usually female is carrier and not affected. • Dosage compensation • One X chromosome is inactivated in every female cell. • Inactivation occurs randomly in early embryo of several thousand cells. • After inactivation, same X is inactivated in daughter cells. Examples: Duchenne muscular dystrophy, hemophilia A and B • There are a few X-linked dominant disorders. • Example- vitamin D-resistant rickets
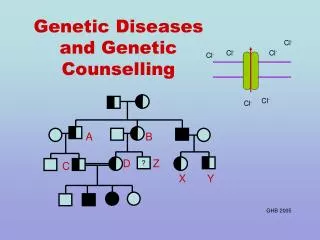
Cytogenetic disorders • Diagnosed by a karyotype • Photograph of stained chromosomes from a metaphase spread arranged in order of decreasing length • Chromosomes are identified by location of centromere and banding pattern • Numerical abnormalities • Polyploid a multiple of n > 2 • Aneuploid (not an exact multiple of n) e.g. trisomy • Structural abnormalities • Chromosome breakage plus loss or rearrangement
Cytogenetic disorders of autosomes • Some trisomies (2n+1) are compatible with survival. • 21, 18, and 13 • Phenotypic abnormalities • Monosomy is not compatible with life. • Rearrangements during gametogenesis result in abnormal (unbalanced) gametes. • Translocations, deletions, isochromosomes, inversions, ring formation • Usually these disorders are de novo.
Down’s Syndrome • Trisomy 21 • Most cases result from meiotic non-disjunction in mother. • In ~ 4% of patients, the extra chromosome is the result of a Robertsonian translocation. • Phenotype: epicanthic folds, mental retardation, 40% have cardiac malformations, increased risk of developing acute leukemia, Alzheimer disease .
Rearrangements of chromosomes resulting in aberrations BP 7-17