Download

1 / 32
320 likes | 652 Views
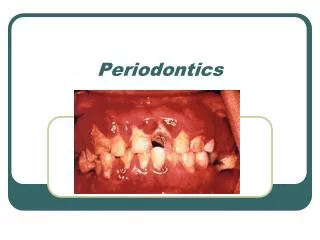
UCLA SCHOOL OF DENTISTRY. Presents. Presents. Dr. E. Barrie Kenney Professor

E N D
5. Many clinicians believe Traumatic occlusion causes Intrabony Periodontal defects but this is not so. This defect is caused by dental plaque with accentuation due to the open contact region and poor subgingival margin of Restoration.
6. Histology of Intrabony defect due to plaque induced Periodontitis. Arrows show sub gingival plaque on root surface
7. Irritation factors are plaque that induces Gingivitis which progresses to Periodontitis. Traumatizing factors from occlusion cause tissue changes in periodontal ligament space.
8. Zone of co-destruction occurs when plaque induced Periodontitis occurs in a tooth that also has Traumatic Occlusion resulting in more severe bone loss than that seen with Periodontitis alone.
9. Host parasite reaction between bacterial plaque and host inflammatory response is the cause of pocket depth and attachment loss. The presence of Traumatic occlusion can accentuate the damage when Periodontitis proceeds apically into the Periodontal Ligament Space.
10. The first reaction to increased occlusal loading is increased vascularity in the Periodontal ligament space. No changes are seen in gingival tissues.
11. Normal Periodontal ligament with normal occlusal forces showing dense collagen fibers attached to bone and cementum with minimal vascularity.
12. With excessive occlusal loading the collagen fibers lose their connections between cementum and bone ,and blood vessels proliferate.
13. This initial increased vascularity results in a more compressible periodontal ligament and increased clinical mobility.
14. Changes in the apical periodontal ligament vascular patterns can also result in increased vasodilation of the pulp with increased sensitivity and pain to Hot and Cold stimuli secondary to Traumatic Occlusion.
15. In Traumatic Occlusion after the initial change of increased vascularity, there is a stimulation of osteoclasts which cause bone loss and a widened periodontal ligament space. This also causes increased tooth mobility.
16. Further effects of Traumatic Occlusion are seen with loss of density of collagen and absence of a functional fiber arrangement.
17. High power view. No collagen fibers adjacent to bone and loss of functional support of Periodontium.
18. Advanced Traumatic Occlusion with minimal Periodontal ligament tissue. An advancing plaque induced Periodontitis can rapidly spread apically in this situation.
19.
20. Periodontal ligament tissues can respond with Traumatic Occlusion changes when a normal periodontium is affected by increased occlusal loading due to bruxing clenching or a high restoration These changes are called Primary Occlusal Trauma or Primary Trauma from occlusion.
21. In teeth with bone loss due to periodontal disease previously well tolerated occlusal loading can become traumatic and cause changes in the periodontal ligament tissues. These changes are called secondary occlusal trauma or secondary trauma from occlusion.
22. Coronal portion of plaque induced Periodontitis with pocket formulation
23. Region of crestal bone showing intrabony pocket due to plaque this is blending with Traumatic Occlusion induced Periodontal ligament changes of loss of collagen and increased vascularity.
24. More Apical region with Traumatic Occlusion changes seen deep in Periodontal tissues apical to Periodontitis.
25.
26. Radiograph of lower Molar with Traumatic Occlusion. Widened Periodontal ligament space on Mesial all the way around the apex with beginning bone loss in furcation (arrows).
27. There is also thickened lamina dura and this tooth has increased mobility.
28. First molar has traumatic occlusion causing the bone loss in the furca. Clinically there is no pocket depth nor Periodontitis in the furcation and so the diagnosis is Traumatic Occlusion and the treatment is occlusal adjustment to reduce occlusal loading.
29. Both premolars have traumatic occlusion and there is an addition Periodontitis related bone loss and pockets on the mesial of the first premolar.
30. Gingival recession is not caused by Traumatic Occlusion but is related to inadequate Keratinized Gingiva and excessive tooth brushing.
31. Wedge shaped defect in root of lower first premolar is due to traumatic toothbrushing and is not related to Traumatic Occlusion
32. �Abfraction� type of root loss like this has not been shown to occur clinically in association with heavy occlusal forces.
33. At time of Periodontal surgery large hyperplastic bone response to heavy occlusal load called Buttressing Bone
34. Buttressing Bone removed during periodontal surgery to facilitate normal contour of gingival tissues.