Download
1 / 28
290 likes | 1.27k Views
Seldinger Cricothyrotomy. 2002 ACP Recert. MORNING ROTATION 08:45 Emergency Advanced Airway 09:15 12 Lead Acquisition 09:45 Pediatric Review 10:30 Break 10:45 What is an OSCE? 11:15 Quality Improvement Initiatives 12:00 Lunch. AFTERNOON ROTATION TIME GROUP 1 GROUP 2 GROUP 3

E N D
Seldinger Cricothyrotomy 2002 ACP Recert
MORNING ROTATION 08:45 Emergency Advanced Airway 09:15 12 Lead Acquisition 09:45 Pediatric Review 10:30 Break 10:45 What is an OSCE? 11:15 Quality Improvement Initiatives 12:00 Lunch AFTERNOON ROTATION TIME GROUP 1 GROUP 2 GROUP 3 13:00 OSCE # 1 OSCE # 2 OSCE # 3 13:20 OSCE # 2 OSCE # 3 0SCE # 1 13:40 OSCE # 3 0SCE # 1 OSCE # 2 14:00 0SCE # 4 OSCE # 5 RECERT 14:20 OSCE # 5 RECERT OSCE # 4 14:40 RECERT OSCE # 4 OSCE # 5 15:00 BREAK BREAK BREAK 15:15 TEST TEST TEST OSCE STATION 1 AIRWAY EMERGENCY (CRIC) OSCE STATION 2 PEDIATRIC ASSESSMENT OSCE STATION 3 CAPNOGRAPHY INTERPRETATION OSCE STATION 4 NEEDLE THORACOTOMY OSCE STATION 5 12 LEAD INTERPRETATION AIRWAY RECERT ORAL BOARD - & EMERGENCY CRIC Based on 6 – 12 (max) Paramedics ! Agenda
What is an Indication for Intubation? • LOC • Obtain / Maintain / Protect Airway • Oxygenation • Positive Pressure Ventilation or control ventilation • Drugs (NAVEL) • Fatigue • Access Tracheal Toilet (suction)
Next Determination ? Once the decision to intubate has been made a then what? • Is it a CRASH intubation? • Death or near death (like “NIKE” “just do it”) • Suction, stylette, lubed ETT, stethoscope, laryngoscope • If Time assess for DIFFICULT intubation using? • LEMON (DO YOU NEED TO LOAD YOUR PATIENT ?)
CRASH AIRWAY • VSA • Pending VSA • Respiratory Arrest • GCS < 5 • Airway compromise (blood / vomit unable to clear) Note: positioning is the number 1 airway procedure to prevent aspiration.
What is Loading your Patient? • LOAD: • Lidocaine • Opiate • Atropine • Depolarizing neuromuscular blocking agent (defasiculating) • The art!!!
List the Steps for Difficult Airway Assessment • L - Look 1 point • E - Evaluate 2 points • M - Mallampati (1 - 4) 2 points • O - Obstruction 2 points • N - Neck 1 point 2 or more equals difficult
Critical Thinking! • What are the advantages of facilitated intubation? • What if sedation has been granted and respiratory arrest occurs and you are unable to get the tube? • What if you cannot ventilate? • Explain why it is possible to be unable to ventilate a previously spontaneously breathing patient. • Don’t paint yourself into a corner.
Airway Review Landmark - 2 fingers
Causes of Obstruction • Foreign Body • Trauma • Edema • Neoplasm • Blood
Foreign Bodies • Food • More common in children • In adults there are typically co-factors • Alcohol • Aging
Fractured Larynx • Blunt trauma • Rapid & severe • Posterior tear • Seldinger Cric can cause expansion of tear • True surgical airway emergency
Emergency Cricothyrotomy Protocol • If a patient cannot be ventilated due to life-threatening suspected upper airway obstruction, the Advanced Care Paramedic may attempt a cricothyrotomy according to the following protocol after receiving orders from the BHP. • Indications: • A patient that requires intubation and • Unable to intubate and • Unable to adequately ventilate • Conditions: • Patient 40 kg and 12 years old • Contraindications: • Suspected fractured larynx • Inability to localize the cricothyroid membrane
Emergency Cricothyrotomy Protocol Procedure: 1. Administer 100% O2. 2. Contact the BHP for on-line medical direction to proceed with this protocol. 3. If every attempt to contact a BHP has failed, the AC Paramedic may continue with this protocol in a life-threatening situation if all other indications and conditions are met. The AC Paramedic should contact the BHP (and the Base Hospital) as soon as possible after the procedure and document the patch failure and decision to proceed. 4. Place patient on his or her back, and then extend the head and neck (provided there are no c-spine injuries). 5. Grasp the larynx with your thumb and middle finger. Locate the cricoid cartilage and the cricothyroid membrane with the index finger. Prep the area quickly. Follow the appropriate procedures following for the specific equipment used. The seldinger cricothyrotomy should be the primary method used but if the equipment is not available, the needle cricothyrotomy procedures should be followed.
Emergency Cricothyrotomy Protocol Seldinger (Melker) Cricothyrotomy Kit: 1. While stabilizing the thyroid cartilage make a vertical incision in the midline of the cricothyroid membrane with a scalpel. 2. Use the supplied 18g TFE catheter with the 6cc syringe attached. Insert the catheter into the airway at a 45º caudal angle looking for free air in the syringe. 3. Remove the syringe and needle leaving the catheter in place. Always maintain contact with the guidewire, never let go! 4. Advance the soft flexible end of the wire guide through the catheter and into the airway several centimeters caudally. 5. Remove the catheter leaving the wire guide in place. (STEP # 1) 6. Feed the dilator (with airway catheter in place) over the wire. Ensure that the stiff end of the wire protrudes out of the back of the dilator. 7. Advance the dilator into the airway until the flange of the 15mm airway adapter is resting against the patient's neck. 8. Remove the dilator and wire guide. Use caution to ensure that the wire guide is not lost into the trachea. 9. Secure the flange of the airway adapter to the patient. 10.Attach a BVM and attempt to ventilate the patient. Genesis or other ventilators must not be used. 11.Initiate rapid transport to the closest appropriate hospital. 12.Patch to the Base Hospital if complications arise or further orders are required.
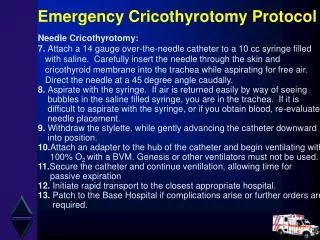
Emergency Cricothyrotomy Protocol Needle Cricothyrotomy: 7. Attach a 14 gauge over-the-needle catheter to a 10 cc syringe filled with saline. Carefully insert the needle through the skin and cricothyroid membrane into the trachea while aspirating for free air. Direct the needle at a 45 degree angle caudally. 8. Aspirate with the syringe. If air is returned easily by way of seeing bubbles in the saline filled syringe, you are in the trachea. If it is difficult to aspirate with the syringe, or if you obtain blood, re-evaluate needle placement. 9. Withdraw the stylette, while gently advancing the catheter downward into position. 10.Attach an adapter to the hub of the catheter and begin ventilating with 100% O2 with a BVM. Genesis or other ventilators must not be used. 11.Secure the catheter and continue ventilation, allowing time for passive expiration 12. Initiate rapid transport to the closest appropriate hospital. 13. Patch to the Base Hospital if complications arise or further orders are required.
Needle Cricothyroidotomy SECOND LINE PROCEDURE that should be used if Seldinger technique is not possible. (BHP may give orders from 8 - 12 year old patient) Provides temporary oxygenation but no ventilation Note: Exhalation may be difficult through such a small diameter catheter and the paramedic should lengthen the time between breaths to allow for exhalation. The BHP may consider giving orders for a second catheter horizontally next to the first to allow for better exhalation and this should be discussed during the patch.
Cricothyroidotomy (Melker) 2 Maintain landmark with one hand & insert the 6cc syringe with 18 guage TFE catheter and introducer needle. Advance needle on a 45° angle to the frontal plane in the midline in a caudad direction. While inserting needle draw back on syringe to verify when trachea has been found. Landmark cricothyroid membrane between the thyroid and cricoid cartilages and prep area.
Cricothyroidotomy 3 4 Remove the syringe and needle leaving the catheter in place. Advance the soft, flexible end of the guidewire through the TFE catheter and into the airway several centimeters. While holding on to the guidewire ensuring not to let it move carefully remove the TFE.
Cricothyroidotomy 6 5 While holding the guidewire make a vertical incision with the # 15 short handle scapel blade to allow dilator to be inserted. While holding on to the guidewire advance the preassembled dilator and airway catheter with the tapered end first over the guidewire.