Download
1 / 10
270 likes | 1.21k Views
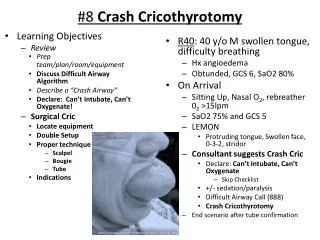
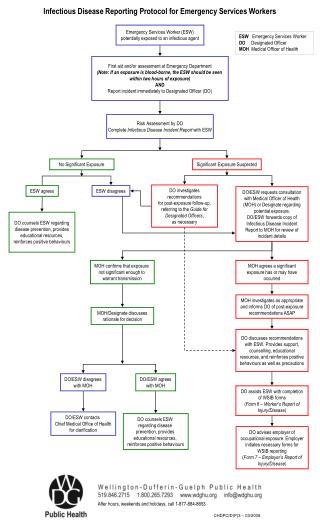
Emergency Cricothyrotomy Protocol. Needle Cricothyrotomy: 7. Attach a 14 gauge over-the-needle catheter to a 10 cc syringe filled with saline. Carefully insert the needle through the skin and cricothyroid membrane into the trachea while aspirating for free air.

E N D
Emergency Cricothyrotomy Protocol Needle Cricothyrotomy: 7. Attach a 14 gauge over-the-needle catheter to a 10 cc syringe filled with saline. Carefully insert the needle through the skin and cricothyroid membrane into the trachea while aspirating for free air. Direct the needle at a 45 degree angle caudally. 8. Aspirate with the syringe. If air is returned easily by way of seeing bubbles in the saline filled syringe, you are in the trachea. If it is difficult to aspirate with the syringe, or if you obtain blood, re-evaluate needle placement. 9. Withdraw the stylette, while gently advancing the catheter downward into position. 10.Attach an adapter to the hub of the catheter and begin ventilating with 100% O2 with a BVM. Genesis or other ventilators must not be used. 11.Secure the catheter and continue ventilation, allowing time for passive expiration 12. Initiate rapid transport to the closest appropriate hospital. 13. Patch to the Base Hospital if complications arise or further orders are required.
Needle Cricothyroidotomy SECOND LINE PROCEDURE that should be used if Seldinger technique is not possible. (BHP may give orders from 8 - 12 year old patient) Provides temporary oxygenation but no ventilation Note: Exhalation may be difficult through such a small diameter catheter and the paramedic should lengthen the time between breaths to allow for exhalation. The BHP may consider giving orders for a second catheter horizontally next to the first to allow for better exhalation and this should be discussed during the patch.
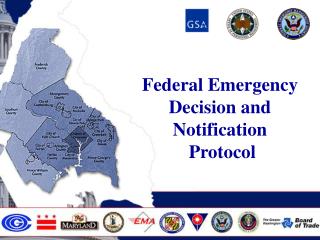
Cricothyroidotomy (Melker) 2 Maintain landmark with one hand & insert the 6cc syringe with 18 guage TFE catheter and introducer needle. Advance needle on a 45° angle to the frontal plane in the midline in a caudad direction. While inserting needle draw back on syringe to verify when trachea has been found. Landmark cricothyroid membrane between the thyroid and cricoid cartilages and prep area.
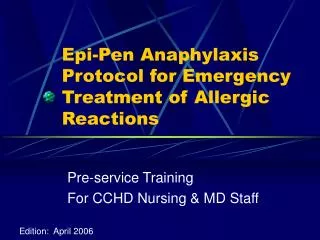
Cricothyroidotomy 3 4 Remove the syringe and needle leaving the catheter in place. Advance the soft, flexible end of the guidewire through the TFE catheter and into the airway several centimeters. While holding on to the guidewire ensuring not to let it move carefully remove the TFE.
Cricothyroidotomy 6 5 While holding the guidewire make a vertical incision with the # 15 short handle scapel blade to allow dilator to be inserted. While holding on to the guidewire advance the preassembled dilator and airway catheter with the tapered end first over the guidewire.
By the way This is the most invasive skill our ACPs may be delegated and therefore a skill that can be done quickly and with precision. When the decision to use this skill has been made the techniques should be accomplished within 1 minute. During this skill assessment you will be allotted 2 attempts to meet this requirement. The mannequin is available during lunch to practice.