Download
1 / 47
490 likes | 974 Views
High-grade Prostatic Intraepithelial Neoplasia on Needle Biopsy Risk of Cancer on Repeat Biopsy Related to Number of Involved Cores and Morphologic Pattern. Tarek Bishara, MD,* Dharam M. Ramnani, MD , # Jonathan I. Epstein, MD.

E N D
High-grade Prostatic Intraepithelial Neoplasia on Needle BiopsyRisk of Cancer on Repeat Biopsy Related to Number of Involved Cores and Morphologic Pattern Tarek Bishara, MD,* Dharam M. Ramnani, MD,#Jonathan I. Epstein, MD. *Pee Dee Pathology Associates, Florence, SC; #Virginia Urology Center, Richmond, VA; and Johns Hopkins Medical Institutions, Baltimore, MD. Am J Surg Pathol · Volume 28, Number 5, May 2004
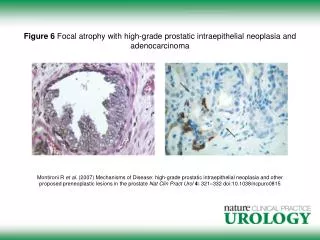
HGPIN • Definition:an abnormal proliferation of prostate ducts and acini with cytologic changes similar to prostatic carcinoma • Importance on needle biopsy: an association with synchronous, occult prostatic adenocarcinoma
HGPIN • Isolated finding on needle biopsy: 0.7% to 24 % (4% to 6%) • Risk of carcinoma in subsequent biopsy: 23% to 79% (23% to 35%, mean= 25.3%) • in a contemporary, PSA-screened population: 10% to 27% • risk of finding cancer after a benign diagnosis on needle biopsy: 11% to 24% (26.2%)
HGPIN • Whether or not a patient should be rebiopsied based solely on an isolated HGPIN diagnosis? • Will clinical factors help in predicting which patients will have prostatic carcinoma on follow-up biopsies? • DRE, serum PSA levels, and transrectal ultrasound findings
METHODS • 200 cases (May 1999 ~ Sep 2002) • 179 cases (89.5%) had available follow-up information • 132 cases (66%%) had ≥ 1 follow-up biopsy
METHODS • Histological subtypes: • tufting / flat • micropapillary / cribriform • Number of cores involved by HGPIN
METHODS • Rebiopsied specimen • benign prostatic tissue • HGPIN • atypical glands • carcinoma
RESULTS • Age: 46-90 years (mean = 66.4) • Interval between initial biopsy and first rebiopsy: 1 to 33 months (mean = 7) • Number of prostatic cores per biopsy set: 4 to 15 • standard 6 core sextant biopsy was obtained in 59.8% of initial biopsies and 61% of follow-up biopsies
RESULTS • Histologic subtypes in initial biopsies • tufting: 59.0% (115 of 195) • micropapillary: 34.3% (67 of 195) • cribriform: 6.2% (12 of 195) • flat: 0.5% (1 of 195) • Extent in initial biopsies • One core: 51.5% (68 of 132) • Two or more cores: 48.5% (64 of 132)
RESULTS • Diagnosis in the follow-up biopsies • Benign prostatic tissue: 45% (60 of 132) • HGPIN: 17.4% (23 of 132) • Atypical glands: 8.3% (11 of 132) • Adenocarcinoma: 28.8% (38 of 132)
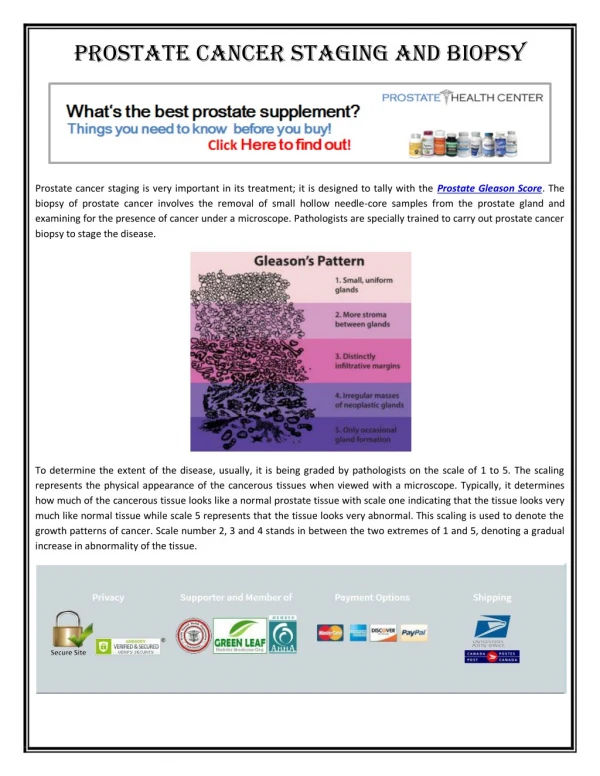
RESULTS • Adenocarcinoma in follow-up biopsies • incidence: 28.8% (38/132) • Interval between repeat biopsy: 2-36 months (mean=10.6) • Gleason score • 5: 5.3% ( 2 of 38) • 6: 89.5% (34 of 38) • 7: 5.3% ( 2 of 38)
RESULTS • Incidence of subsequent carcinoma • tufting / flat: 31.9% (29/91) • micropapillary / cribriform: 22.0% (9 of 41) • p = 0.244
RESULTS • Incidence of subsequent carcinoma • 1 core with HGPIN: 22.0% (15/68) • ≥ 2 cores with HGPIN: 35.9% (23 of 64) • p = 0.078
RESULTS • Adenocarcinoma in follow-up biopsies • 1st follow-up biopsy: 71.1% (27 of 38) • 2nd follow-up biopsy: 18.4% (7 of 38) • 3rd follow-up biopsy: 10.5% (4 of 38) • 4th follow-up biopsy: 2.6% (1 of 38) • All had abnormal diagnoses on at least one of the previous biopsies
RESULTS • Incidence of subsequent carcinoma • Benign diagnosis on the 1st follow-up biopsy (n=36): 14.3 % (2 of 14) • HGPIN on the 1st follow-up biopsy (n=25): 32.0% (8 of 25) • Small atypical glands on the 1st follow-up biopsy (n=6): 33.3% (1 of 3)
RESULTS • Incidence of subsequent carcinoma • Multiple cores involved by HGPIN on the 1st follow-up biopsy: 50.0 % (8 of 16) • Only one core involved by HGPIN on the 1st follow-up biopsy: 0 % (0 of 9) • p = 0.01
RESULTS • If one combined the risk of cancer on repeat biopsy for those men with either no HGPIN or one core with HGPIN on first repeat biopsy as compared with men with multiple cores of HGPIN on repeat biopsy, the result was more significant (P = 0.008).
Widespread High-grade Prostatic Intraepithelial Neoplasia on Prostatic Needle Biopsy: A Significant Likelihood of Subsequently Diagnosed Adenocarcinoma George J. Netto, MD. and Jonathan I. Epstein, MD.* Departments of Pathology, *Urology, and*Oncology, The Johns Hopkins Hospital, Baltimore, MD. Am J Surg Pathol 2006;30:1184–1188
MATERIALS & METHODS • 73 cases (1994 ~ 2005) • Prostatic needle biopsy • Diagnosis of HGPIN in a minimum of 4 cores
MATERIALS & METHODS • 73 cases • 41 cases had at least one follow-up biopsy • age: 66.8 years • numbers of initial cores: 10.4 • PSA: 2.5-90 ng/mL (mean=14.1; median=8.2) • 32 cases were lack of follow-up biopsy • age: 68.2 years • numbers of initial cores: 10.4 • PSA: 0.5-8.5 ng/mL (mean=3.5; median=3.3)
MATERIALS & METHODS • Data of follow-up samples • Date • Nature • Frequency
MATERIALS & METHODS • Diagnosis of follow-up samples • benign prostatic tissue (BPT) • HGPIN HGPIN with adjacent small atypical glands (PINATYP) • carcinoma (PCa)
MATERIALS & METHODS • Statistics • STATA, College Station, TX • Student t test to assess potiential differences in age and number of cores sampled between those men with and without repeat biopsy • X2 test to assess differences between subgroups among men who had a repeat biopsy
RESULTS • Age: 66.8 years • Period of follow-up: 1-41 months (mean=11) • Numbers of cores on initial biopsy: 5-16 (mean=10.6; median=10) • Numbers of cores on follow-up biopsy: 6-16 (mean=10.4; median=10)
RESULTS • Follow-up biopsy • 1 repeat biopsy: 34 p’ts • 2 repeat biopsies: 3 p’ts • 1 repeat biopsy followed by 1 TURP: 1 p’t • 1 repeat biopsy followed by 2 TURPs: 1 p’t • 1 TURP: 3 p’ts
RESULTS • All but 1 of the prostate cancers were identified on the first F/U procedure • All but 1 of the prostatic carcinomas were diagnosed within 2 years from the initial biopsy with 10 rendered within the first year
RESULTS • Adenocarcinoma in follow-up biopsies • incidence: 39% (16/41) • time from the initial biopsy: 1-36 months (mean=10.4) • Gleason score • 5: 6.3% ( 1 of 16) • 6: 68.7% (11 of 16) • 7: 18.8% ( 3 of 16) • 9: 6.3% ( 1 of 16)
RESULTS • 5 p’ts with more than 1 f/u biopsies • 1st f/u biopsy (negative) --> TURP (PCa) • 1st and 2nd f/u biopsies (HGPIN) • 1st f/u biopsy (HGPIN) --> biopsy (PINATYP) • 1st f/u biopsy (PINATYP) --> biopsy (HGPIN) • 1st f/u biopsy (PINATYP) --> TURP (BPT) --> TURP (BPT)
DISCUSSION • The reported likelihood of finding cancer after a diagnosis of HGPIN on needle biopsy has decreased in the contemporary era. • Seven of nine large studies showed no statistically significant difference in the risk of cancer on repeat biopsy after an HGPIN diagnosis compared with rebiopsy after a benigndiagnosis.
DISCUSSION • Herawi M, et al. Risk of prostate cancer onre-biopsy following a diagnosis of high-grade prostatic intraepithelial neoplasia (HGPIN) is related to the number of cores sampled. J Urol. 2006;175:121–124. • In cases with 6 core biopsies for both the initial and rebiopsy, the risk of cancer after HGPIN was 14.1% (20/142) • With an initial 6 core biopsy and >8 core repeat biopsy, the risk increased to 31.9% (36/113) • With >8 core biopsy sampling for both the initial and repeat biopsies, the risk for cancer was 14.6% (37/253)
DISCUSSION • Delaying the repeat biopsy allowing for a longer interval than the originally recommended 6 to 12 months • Identifying a subset of HGPIN patients with a higher subsequent PCa risk
DISCUSSION • Our study demonstrated a 39% likelihood of finding PCa after the initial identification of widespread (4 or more HGPIN) • The 39% likelihood rate stands in significant contrast to the baseline risk (19% to 26.2%) of finding adenocarcinoma on a repeat biopsy after an initial benign diagnosis.
DISCUSSION • All but 1 cases of the adenocarcinoma diagnoses were obtained at the first F/U procedure. The absolute need for a second repeat biopsy after a first negative repeat biopsy could be questioned.
SUMMARY • An initial finding of HGPIN on 4 or more cores • Patients older than 70 years of age • Patients with a fewer numbers of cores on initial biopsy