Download
1 / 5
60 likes | 239 Views
Biopsy of recurrence in breast cancer. Immunohistochemistry discrepancy between prymary tumor and metastases. Hormonal receptors discrepancy around 40% Also different profile for HER-2 marker Most of the studies are retrospectives on design. J Clin Oncol 30:587-592 2012.

E N D
Biopsy of recurrence in breast cancer Immunohistochemistry discrepancy between prymary tumor and metastases. • Hormonal receptors discrepancy around 40% • Also different profile for HER-2 marker • Most of the studies are retrospectives on design J Clin Oncol 30:587-592 2012
The NCCN Panel recommends that metastatic disease at presentation The NCCN Panel recommends that metastatic disease at presentation The NCCN Panel recommends that metastatic disease at presentation or first recurrence of disease should be biopsied as a part of the workup or first recurrence of disease should be biopsied as a part of the workup or first recurrence of disease should be biopsied as a part of the workup The NCCN Panel recommends that metastatic disease at presentation or first recurrence of disease should be biopsied as a part of the workup for patients with recurrent or stage IV disease. This ensures accurate determination of metastatic/ recurrent disease and tumor histology, and allows for biomarker determination and selection of appropriate treatment. Efforts should be made to obtain histopathological confirmation whenever technically feasible, particularly in the situation of an isolated metastatic lesion. Biological markers important for treatment decisions, such as steroid hormone receptors (ER, PR) and HER-2 status should be re-evaluated, at least once, in a metastatic lesion. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf for patients with recurrent or stage IV disease. This ensures accurate for patients with recurrent or stage IV disease. This ensures accurate for patients with recurrent or stage IV disease. This ensures accurate determination of metastatic/ recurrent disease and tumor histology, and determination of metastatic/ recurrent disease and tumor histology, and determination of metastatic/ recurrent disease and tumor histology, and
What is the eviddence? HER2 discordance between primary breast cancer and its paired metastasis: tumor biology or test artefact? Insights through meta-analysis Nehmat Houssami, Petra Macaskill, Rosemary L. Balleine, Michael Bilous,Mark D. Pegram 2520 patints, 26 retrospectives studies. Discordancy ratio: 5.5% (3.6 -8.5%) Major discrepancy between initial diagnosis and metastases, less for regional nodes. (4.1% vs 3.3%) Breast Cancer Res Treat 129, 659-674 (2011)
More evidence DESTINY
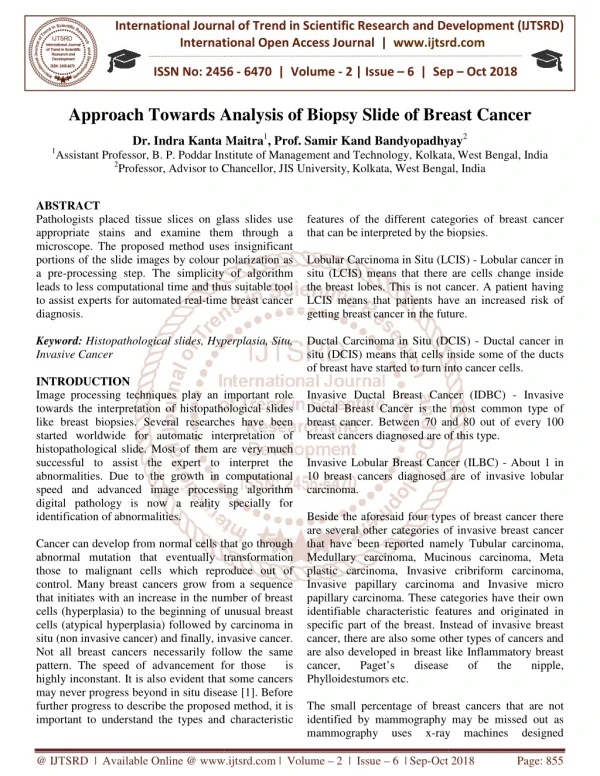
Proposed algorithm for biopsy of recurrence in breast cancer The Oncologist 2010: 15: 1164-1168 Nature Reviews Clin Oncol 2013