Download
1 / 33
800 likes | 3.6k Views
Assessment and Management of Strabismus. Fiona Crotty Head Orthoptist East Sussex Hospitals. Overview. Development of Visual Acuity Assessment of Vision in Infants & children What is BSV and how does it develop? Classification of squint Assessment of squint Management of squint.

E N D
Assessment and Management of Strabismus Fiona Crotty Head Orthoptist East Sussex Hospitals
Overview • Development of Visual Acuity • Assessment of Vision in Infants & children • What is BSV and how does it develop? • Classification of squint • Assessment of squint • Management of squint
Development of Visual Acuity • Dependent upon normal anatomical and physiological development • Eye relatively well developed in full-term infant • Shorter axial length (more hypermetropic) • Shallow anterior chamber • Poorly differentiated fovea (complete by 4 months age) • Accommodation 90% accurate by 2 – 3 months
Development of Visual acuity (VEP’s) * Tested with single optotypes
Assessment of Vision Birth to 12 months – forced choice preferential looking
Assessment of Vision – LogMAR vs. Snellens Type • Snellens: • Traditional method • 6 metre test distance • Recorded as fraction e.g.6/60, 6/9 • Inconsistent numbers & spacing of letters per row • logMAR: • Decimal value, 0.0 =6/6 equivalent, 0.2 = 6/9.5 etc • Equal number of letters per row, consistent spacing • Greater range of acuity values & can be used at 3m • Preferred method for research and amblyopia testing
Assessment of Vision Snellens Chart logMAR Chart
What is BSV? • Definition of Binocular Single Vision (BSV) • The ability to use both eyes simultaneously so that each eye contributes to a common single perception • 3 levels • Simultaneous perception ( 2 images seen) • Fusion (Interpreting 2 images as one) • Stereopsis (3-D appreciation)
Development of BSV • Newborn reflexes present – essential for BSV development • Require continued use and normal visual experience • Postural reflexes: static (head position to body) and stato-kinetic (head relative to space) • Fixation reflexes: fixation (foveal) and re-fixation (target to target and maintained to moving object)
Development of BSV Most neonates show coarse re-fixation • Conjugate fixation 1st to develop (eyes follow object together) • Disjugate fixation (follow approaching object – convergence) • Fusional reflex (correct for change in image position) • Kinetic reflex (controlled accommodation & convergence)
Development of BSV • From aet 4/52 Attempts at convergence seen • 5-6/52 conjugate fixing and brief following – neonatal misalignment common • 4/12 saccadic eye movements develop, neonatal misalignments reduce • 6/12 – 8/12 normal BSV established
Risk Factors for Development of Squint • Prematurity • Neuro-developmental delay • Motor control disorders eg cerebral palsy • Refractive error, failure to emmetropise • Family history
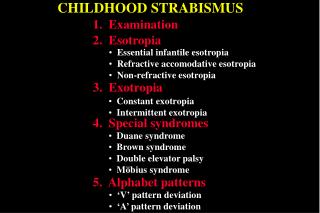
(Brief) Classification of Squint • Manifest (Heterotropia) • Esotropia (convergent) • Exotropia (divergent) • Vertical • Unilateral or alternating • Constant or intermittent (in Primary position, or in certain positions of gaze) • Accommodative
(Brief) Classification of Squint • Latent (Heterophoria) • Esophoria • Exophoria • Vertical ‘phoria • Fully compensated • Poorly compensated
Assessment of squint • Visual Acuity • Cover Test • Ocular Movements • Convergence • Fusion/Stereopsis? • Measurement of angle (prisms)
Management of Squint • Orthoptic assessment • Cycloplegic refraction & fundoscopy • Correct significant refractive error • Allow for refractive adaptation (up to 18/52) • Occlusion treatment for amblyopia (patches, atropine) • Orthoptic exercises (intermittent deviations) • Surgery
Summary • Early intermittent neonatal misalignment common between birth and 2-4 months • BSV well established from 6 months • Sensitive period for development of vision and binocular reflexes • Suspected squint after 4 months (corrected) age should be referred for Orthoptic assessment
Acknowledgements • Thank you to Manuel Saldana for his kind permission to use the video clips