Download
1 / 21
210 likes | 487 Views
Combining pills to improve the experience of multiple pill taking: a qualitative study of people with hypertension and raised cholesterol B Williams, R Durrant, University of Dundee. C Pagliari , University of Edinburgh.

E N D
Combining pills to improve the experience of multiple pill taking: a qualitative study of people with hypertension and raised cholesterol B Williams, R Durrant, University of Dundee. C Pagliari, University of Edinburgh. I Crinson, A Shaw, S de Lusignan, St. Georges Hospital Medical School, London Funded by Pfizer UK.
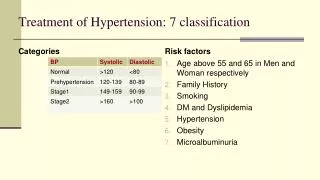
Background • Hypertension & Cholesterol • Age & co-morbidities • Complexity of drug regimens • Medication taking & adherence
Background • Combining tablets • Swallowing • Procedural complexity • Attitudes to combined tablets unknown • How would it fit with current self-care strategies?
Aim To explore attitudes and practices to medication regimes among patients already in receipt of multiple medications, and to assess whether a combined tablet would be perceived as advantageous
Methods • Design: • 14 Focus groups: 8 in Scotland, 6 in England • Sample: • 92 people, age >45 yrs, hypertension AND raised cholesterol • Data collection: • Topic guide, illness beliefs, practices & attitudes, combined pill. • Analysis: • Recorded, transcribed, “Framework”, NVivo.
Experience & Concerns • Discomfort • Organisation • Packaging • Swallowing • Side-effects • Anxieties • Dislike of “chemicals in the body” • Interactions • Addiction
Frank (69 yrs): I wonder if we’re addicted to these tablets. We’ve been taking them for so long…….My doctor, Dr Harris, he’s a good chap, I quite like him. He said to me prevention – take them, and then it won’t come. Do without them and it’ll come. Tom (65 yrs): Well that is going to get addicted to them if you’re going to do that then. Frank: Well that’s what he said to me, prevention. Tom: You’d be as well saying you're a druggie if you start doing that.
Drug numbers & complexity • Ingredients of complexity: • Numbers of tablets, medications, combinations, doses, times of day. • Routine • Routines within routines – self-care algorithm • Anchor points • Simplification and complication as solutions
Anthony (52 yrs):…..the only problem I have with the blood pressure tablets and the statin that I take, is my change-around period where I go from night shift to an early shift. Now you have to take them before you go to sleep but over the weekend I have to go through a period where I don’t take statin and I don’t take blood pressure pills for the simple reason it would be too much in one period so I go through probably an eight hour period where I am catnapping wide awake but just……….
Threats to Routine • Stability of prescribing • Medications • Doses • Appearance • Stability of domestic anchor points
The Bind Increased complexity requires increased routine But Increased complexity makes routine less likely through increased instability of prescribing and increased vulnerability to changes in daily anchor points
A combined pill? • Initially positive • Convenience • Reduce errors • Less to remember • Cheaper • Initially negative • Tablet size • Allergies/reactions • Attribution of side-effects • Increased consequence of errors • Reduction in potential flexibility
And then…….. Widespread rejection
Wendy (60 yrs): I think it would be wonderful but I can’t see it working because you know you’re, I mean I was on 100 mgs of one drug, they done a blood test and they dropped me down to 75 so you’re going to be changing it all the time…..they chop and change. Nigel (66 yrs): I don’t honestly think so because there are different heart tablets and different cholesterol tablets and it is difficult enough to find the one that suits you rather than suddenly finding that they put two together and you can’t find one that suits you. If they were asking for a recommendation then I would say no.
Problems….. • Availability of matching combinations • Willingness to trade-off • Titration
Conclusion • FDCs may not support self-care • Self-management can mean good complexity • Supporting self-care means supporting stability
Epilogue • Would people with hypertension and raised cholesterol still take a combined pill despite these concerns? • Follow-up survey of 1,400 patients (63 questions, 71% response rate) • Initial findings confirm qualitative study • But……..
The Lesson • People on multiple medications may be self-managing well even if they are technically non-adherent. • They may have fears and concerns about combined pills but the doctor/practitioner rel’p may mask these. • Acceptance of a prescription should not be taken to mean it is not problematic to the patient – and it may damage established self-care behaviours.