Download
1 / 28
280 likes | 409 Views
Family Health Program Brazil Coverage and access. Aluísio J D Barros Andréa D Bertoldi Juraci Cesar Cesar G Victora Epidemiologic Research Center, UFPel Pelotas, Brazil. Centiles of income distribution in Brazil. Values in US dollars. Data: Sample from 2000 Census, IBGE.

E N D
Family Health ProgramBrazil Coverage and access Aluísio J D Barros Andréa D Bertoldi Juraci Cesar Cesar G Victora Epidemiologic Research Center, UFPel Pelotas, Brazil
Centiles of income distribution in Brazil. Values in US dollars. Data: Sample from 2000 Census, IBGE. Brazil: country of inequalities • Among the highest in income concentration • Gini = 60.7 • Important differences across economic levels in • health • education • employment
The Brazilian “Unified Health System” • Created by the 1988 Constitution • Universal system • covering everyone independent of contribution • offering preventive and curative care • simple and complex • decentralized at municipal level
Standard primary care • Traditionally based on health centers • Loose regional coverage • Team including • a few doctors (part-time) • clinician, pediatrician, gynecologist • nurses and clerical staff • Low salary levels
Family health program - PSF • Health facility with clear geographic coverage • Team formed by • full-time general practitioner • registered nurse • nurse • 4 community health workers • Look after 1000 families (~3000 people) • Competitive salary levels
PSF implementation • Initially deployed in • areas not covered by a health center • poorest areas • Next, existing health centers turned into PSF units • Eventually, all primary health care to be based on PSF • Ministry of Health estimate: • ~35% population covered
Main objectives • Estimate the what proportion of the covered population is poor (focus); • Estimate the percentage of the poor covered by the program (coverage); • Estimate the proportion of the covered population that uses the PSF as their primary source of health care.
Data sources • Site 1: Porto Alegre City (2003) • State capital in South Brazil • population = 1.3 million • x-sectional study with covered population • Site 2: Sergipe State (1999) • Poor state in Northeast Brazil • population = 1.8 million • population-based x-sectional study
Porto Alegre 62 units 56 operating for more than 6 months covered population ~ 140.000 mainly poor peripheral areas growing fast Sergipe 69 out of 75 municipalities covered ~ 70% population govnm’t estimate 400 units operating runs in parallel with Community Health Worker program PSF + PACS = 3000 CHWs PSF status
Porto Alegre x-sectional survey on areas covered by PSF all ages 45 PSF units x 20 households 900 households = ~3000 individuals Sergipe x-sectional survey in areas covered by CHW only children < 5 yrs 30 x 6 x 22 = 3960 households ~ 1900 with at least 1 child < 5 yrs Methods
Porto Alegre wealth index created using 2000 Census sample variables decile cutpoints calculated for POA possible to classify the survey sample using the city population as reference (or state, country) Sergipe principal components assets + schooling of head of hh’d population divided into quintiles variables not compatible with the national index used in POA Economic classification
Data collection - similar • structured interviews with pre-coded questionnaires • interviewing at home • about • financing and expenditure • utilization of health services • access to services • evaluation and opinions about PSF (POA) • morbidity, antenatal care, immunization (SE)
Results: Porto Alegre Study Residents of all ages in an area covered by PSF
Coverage of the poor • ~ 19.3% of the poor in POA are covered by the PSF • overall coverage ~11%
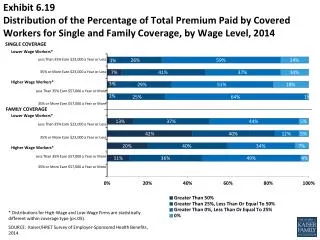
PSF focus* • 36% of sample in Q1 = focus • sample clearly poorer than the city population • <5% in Q5 *Covered individuals are those living in the PSF areas.
PSF focus** **Covered individuals are those who actually used the PSF in the previous 6 months.
Health service utilization • ~ 27% population sought a health service in previous 15 days • Women more than men • Children and elderly more than teens and adults • No difference by economic level • 94% succeeded in getting attention
Results: PSF in Sergipe Children < 5 years-old
PSF focus Economic distribution among those who use the PSF
No antenatal care CI=-42.1 Concentration curve No antenatal care by economic level
Inadequate* antenatal care CI=-18.4 Inadequate antenatal care by economic level Concentration curve *Adequate = at least 6 consultations starting in the first 3 months of pregnancy
Conclusions I • Coverage by PSF still low, especially in Porto Alegre • Access to health services is high • SHS and PSF probably responsible for high access among the poor • PSF focus on the poor is compatible with the implementation strategy and decreases as the program increases its coverage
Conclusions II • Despite universal access, the rich opt out of the system • Coverage by health insurance also decreases use of PSF as primary source of attention • ease of access? • higher quality in the private system?
Conclusions III • Equality in general access is not matched by equality in coverage by programs such as antenatal care • Important inequalities in the adequacy of antenatal care • Two components? • lower quality of public services • public users seek less and demand less from the program
Policy implications • Need to monitor program coverage (incidence) among different social groups through low-cost surveys • Focus on how to improve • quality of services • preventive services in PSF • Need to feed back information to policy makers