Download
1 / 28
340 likes | 922 Views
Strongyloides stercoralis. Clinico-Pathologic Correlation Dr. Christina Day. CLINICAL HISTORY. 54 yo Male with Hx of DM, ESRD and right sided renal transplant in Oct. 2003. BIB EMS with a 1 day Hx of left lower chest “gas” pain radiating to the back and lower abdomen.

E N D
Strongyloides stercoralis Clinico-Pathologic Correlation Dr. Christina Day
CLINICAL HISTORY • 54 yo Male with Hx of DM, ESRD and right sided renal transplant in Oct. 2003. • BIB EMS with a 1 day Hx of left lower chest “gas” pain radiating to the back and lower abdomen. • Associated symptoms included; nausea, vomiting, chills, bloating lethargy, anorexia and shortness of breath.
MEDICATIONS • Immunosupressive therapy: • Rapamune, FK-506, Corticosteroids • Warfarin • Lasix • Lipitor • Minocyclin • Nexium • Bactrim
PHYSICAL EXAM • Genaral: Mod. distress, Pain 5/10, afeb • CVS: Tachycardic, regular, no murmurs • Respiratory: Pox 92%, CTAB • Abdomen: • Moderate-severe tenderness • +Rebound and voluntary guarding • Guiac +
LABS • WBC- 11.3, Na+-122, K+-5.8, BUN-51, Cr-3.1, Glucose-269 • Autoimmune w/u- Negative (except lupus anticoagulant +) • Sputum cytology initally negative • Rapamune/FK-506 in theraputic range • ESR-59, Fibrinogen-671, D-dimer –neg • PSA- 9.7
IMAGING • 1/29/04 • CXR: negative • Abdo XR: thick loops of small bowel in RUQ, edema vs. hemorrhage, no obstuction • 2/2/04 • CXR: ?ARDS with bilateral infiltrates, ?diffuse alveolar hemorrhage
CINICAL COURSE • 1/29: Pt kept NPO, Abx started with impression of Rapamune induced enteritis vs. infective. • 1/30: Febrile with afib. Cr >3, Rapamune held, ? Induced gastritis. • 1/31: Resp. distress and hemoptysis, b/l rals. Impression- pulmonary edema and hemoptysis secondary to NGT. DDAVP given and Warfarin held.
CINICAL COURSE (cont.) • 2/1: Rapid Afib, resp. distress requiring intubation with frank blood on suctioning. Transfused PRBC and FFP. • 2/2: Intermittent Afib. Impression of ARDS with diffuse alveolar hemorrhage. • 2/3: Episodes of de-sats, hypotension and tachy. Large clots on suctioning. Cardiac arrest with failed resuscitation. Pt pronounced dead at 4:55am.
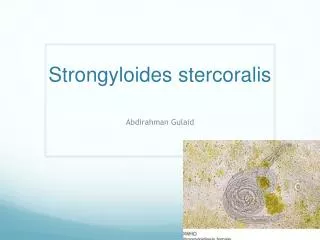
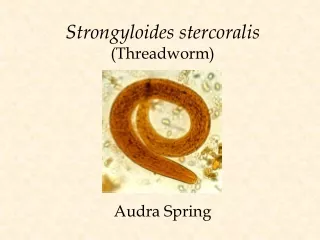
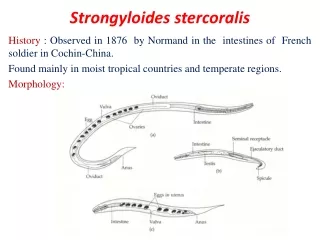
STONGYLOIDES STERCORALIS • Free living parasitic nematode of the small intestine of humans and animals. • Adult females as large as 2.7mm • Live deep in crypts of duodenum and lay eggs rhabditoid larvaefecal excretion infective larvae in soil penetrate skin travels to lungs and intestine via blood adult females.
S. Stercoralis in Immunocompromised Host • Rhabditoid larvaeinfective filariform larvae within the intestinere-enter the blood through the intestinal wall lungssmall intestine. • This second phase of development is know as autoinfection. When massiveHyperinfection. • Explains longevity of infection in humans know to be up to 40 years in some patients.
Clinical Course of Infection • Majority of infected immunocompetent hosts have no symptoms. • How S.stercoralis produces symptoms is unknown. • Hyperinfection occurs in patients with: organ transplant, some lymphoid tumors, prolonged steroid treatment, malnutrition. • NOT associated with HIV infection.
Symptoms and Signs of Hyperinfection • Diarrhea • Abdominal pain • Can mimic peptic ulcer or duodenitis • SOB • Pleuritic pain • Peripheral eosinophilia
Morphologic Changes • Usually minimal in duodenum, edema and hyperemia with hyperinfection. • Colon with ulcerations of various size. • Lungs are heavy, consolidated and hemorrhagic.
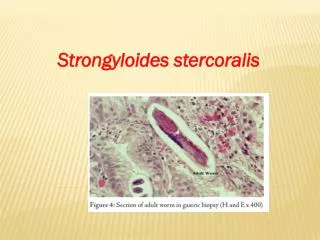
Microscopic findings • Intestine shows adult worms, eggs and larvae. • Lungs and other organs show only larvae.
Diagnosis • Clinical lab finding rhabditoid larvae in stool. • With hyperinfection • filariform larvae may be recovered in stool if fixed rapidly. • Sputum samples • Other body fluids and tissue may also yield larvae.